You might also like
- Forensic ToxicologyDocument27 pagesForensic ToxicologyMarkus WolfeNo ratings yet
- Week 8and 9powerpoint SLP Forensic ChemistryDocument60 pagesWeek 8and 9powerpoint SLP Forensic ChemistrySheena De Guzman MorenoNo ratings yet
- Forensic ToxicologyDocument10 pagesForensic ToxicologyArchie ToribioNo ratings yet
- Learning Module 5 - Forensic ChemDocument22 pagesLearning Module 5 - Forensic ChemjohnNo ratings yet
- Unit 2 Poisons and PoisoningDocument16 pagesUnit 2 Poisons and PoisoningKhar Mel GoNo ratings yet
- Forensic Toxicology: DR Sagal Omar Anatomical PathologistDocument16 pagesForensic Toxicology: DR Sagal Omar Anatomical PathologistCabdiNo ratings yet
- CHAPTER 4 CAUSES OF DEATH and SPECIAL DEATHSDocument10 pagesCHAPTER 4 CAUSES OF DEATH and SPECIAL DEATHSJm LanabanNo ratings yet
- Forensic ChemDocument28 pagesForensic ChemAries Gallandez100% (4)
- Forensic Drug Analysis: 60 % of Forensics Lab Work Is DrugsDocument22 pagesForensic Drug Analysis: 60 % of Forensics Lab Work Is DrugsSaeed KhawamNo ratings yet
- Forensic Toxicology HDocument18 pagesForensic Toxicology Hq_onda_fhonixNo ratings yet
- Week 10 - Forensic ChemistryDrugsToxicologyDocument120 pagesWeek 10 - Forensic ChemistryDrugsToxicologycuambyahoo100% (1)
- Forensic Toxicology Drug TestingDocument53 pagesForensic Toxicology Drug TestingNarciso Ana Jenecel100% (1)
- Forensic Toxicology Powerpoint 1Document18 pagesForensic Toxicology Powerpoint 1api-336788650100% (2)
- New Cur Forensic Chemistry and ToxicologyDocument77 pagesNew Cur Forensic Chemistry and ToxicologyJeaniel Joy Babol BS CRIMNo ratings yet
- Toxicology Drug AnalysisDocument7 pagesToxicology Drug AnalysisAnna Marie Ventayen Miranda100% (1)
- Forensic Toxicology: Most Reported and Fatal PoisoningsDocument165 pagesForensic Toxicology: Most Reported and Fatal PoisoningsAnonymous 6QBs1MSiNo ratings yet
- Forensic Chem Lec ModuleDocument69 pagesForensic Chem Lec ModuleSamantha MendozaNo ratings yet
- Forensic Medicine Lecture on Scene of Death InvestigationDocument9 pagesForensic Medicine Lecture on Scene of Death InvestigationAzra AzmunaNo ratings yet
- Forensic ChemistryDocument9 pagesForensic ChemistryJose Li ToNo ratings yet
- Forensic Microscopy TechniquesDocument8 pagesForensic Microscopy TechniquesCL SanchezNo ratings yet
- Boholst, Jewerly Mae Forensic Chemistry &toxicology B.S Criminology 3 Year / Block ADocument8 pagesBoholst, Jewerly Mae Forensic Chemistry &toxicology B.S Criminology 3 Year / Block AJewerly BoholstNo ratings yet
- Forensic Toxicology: Maria Paula Mayorga Colorado Cód. 1015480095 TK1Document8 pagesForensic Toxicology: Maria Paula Mayorga Colorado Cód. 1015480095 TK1MariaPaulaMayorgaColoradoNo ratings yet
- Gun Shot ResidueDocument21 pagesGun Shot ResidueHannah Jean EstebanNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic Toxicologyapi-3763814100% (5)
- CRMTC5 Legal MedicineDocument19 pagesCRMTC5 Legal MedicineARBE NOVICIONo ratings yet
- Forensic Chemistry - Laboratory Manual ANDREWS 2001 PDFDocument75 pagesForensic Chemistry - Laboratory Manual ANDREWS 2001 PDFjavier chavezNo ratings yet
- Experiment 6 Gunpowder-2Document3 pagesExperiment 6 Gunpowder-2HK FreeNo ratings yet
- Blood Spatter LabDocument10 pagesBlood Spatter Labwalt richardsNo ratings yet
- Medico-Legal Death Investigation StagesDocument29 pagesMedico-Legal Death Investigation StagesColleen Rose Guantero100% (1)
- Forensic ChemistryDocument11 pagesForensic ChemistryBEST OF ONE PIECENo ratings yet
- Police Photography (BIGWAS)Document15 pagesPolice Photography (BIGWAS)KARLVINNo ratings yet
- Victorious Training and Review Center CriminalisticsDocument41 pagesVictorious Training and Review Center CriminalisticsArgie DionioNo ratings yet
- Forensic ScienceDocument11 pagesForensic ScienceLokesh Jindal75% (4)
- College of Criminal Justice Education: Forensic Chemistry and Toxicology - Forensic 3Document17 pagesCollege of Criminal Justice Education: Forensic Chemistry and Toxicology - Forensic 3Rheylyn Mae ValleNo ratings yet
- F ToxicologyDocument17 pagesF Toxicologyempress venus bonillaNo ratings yet
- Crim 177Document187 pagesCrim 177Cinja Shidouji100% (1)
- Hairs and FibersDocument16 pagesHairs and Fibersapi-262815720No ratings yet
- 1.forwarding Note For CFSLDocument2 pages1.forwarding Note For CFSLGiri ChouganiNo ratings yet
- An Introduction To Instrumental Methods PDFDocument4 pagesAn Introduction To Instrumental Methods PDFReagan Go100% (1)
- Blood Evidence Techniques: Locating, Collecting & Preserving Blood SamplesDocument21 pagesBlood Evidence Techniques: Locating, Collecting & Preserving Blood SamplesEmelie TipayNo ratings yet
- Introduction To ForensicsDocument64 pagesIntroduction To ForensicsMarkus Wolfe83% (6)
- Fingerprint Techniques ManualDocument36 pagesFingerprint Techniques ManualAnonymous jGdHMEODVmNo ratings yet
- Lie Detection and Interrogation Reviewer 5Document2 pagesLie Detection and Interrogation Reviewer 5Clarito Lopez100% (1)
- LM5 Medico Legal Aspects of DeathDocument58 pagesLM5 Medico Legal Aspects of DeathRaffy LopezNo ratings yet
- Polygraphy: Prepared By: Group I Palapar (Leader) Prudente Navilla Resurrection SanchezDocument32 pagesPolygraphy: Prepared By: Group I Palapar (Leader) Prudente Navilla Resurrection SanchezAlma AbuacanNo ratings yet
- 1 Nat Sci 12 - Forensic ChemistryDocument7 pages1 Nat Sci 12 - Forensic ChemistryJoselly Floret Salvaloza100% (2)
- Forensic Chemistry Lecture 2Document34 pagesForensic Chemistry Lecture 2CDT LIDEM JOSEPH LESTERNo ratings yet
- Week 11 Powerpoint SLP Forensic ChemistryDocument52 pagesWeek 11 Powerpoint SLP Forensic ChemistrySheena De Guzman MorenoNo ratings yet
- CriminalisticsDocument85 pagesCriminalisticsMS Zhou Si ViolonNo ratings yet
- Forensic biological evidence analysisDocument74 pagesForensic biological evidence analysisMichelle Quiquino Foliente100% (1)
- Forensic Chemistry and Its ApplicationsDocument16 pagesForensic Chemistry and Its ApplicationsKate Aisle EnriquezNo ratings yet
- Legal Medicine - Deception DetectionDocument17 pagesLegal Medicine - Deception Detectionwhisper13941No ratings yet
- Chapter 6 ToxicologyDocument51 pagesChapter 6 ToxicologyRoxana MihaiNo ratings yet
- Examination of Blood StainsDocument54 pagesExamination of Blood Stainsiram khanNo ratings yet
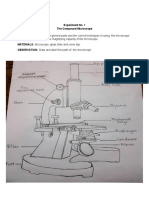
- Using the Compound MicroscopeDocument5 pagesUsing the Compound MicroscopeEarl JohnNo ratings yet
- Module 1 Forensic Chemistry and Toxicology 4Document42 pagesModule 1 Forensic Chemistry and Toxicology 4Aries OlarteNo ratings yet
- Glass Evidence: by The End of This Chapter You Will Be Able ToDocument15 pagesGlass Evidence: by The End of This Chapter You Will Be Able ToArundeep Singh100% (1)
- Methods and Examination of Residues of Gunpowder, Explosion, and Explosive MaterialsDocument3 pagesMethods and Examination of Residues of Gunpowder, Explosion, and Explosive MaterialsEmelie TipayNo ratings yet
- Forensic ToxicologyDocument7 pagesForensic ToxicologyLaiba Jahangir100% (2)
- TOXICOLOGYDocument15 pagesTOXICOLOGYfahadmama47No ratings yet
- Violent Asphyxial DeathsDocument188 pagesViolent Asphyxial DeathsARIF-UR-REHMAN86% (14)
- Regional INJURIESDocument75 pagesRegional INJURIESARIF-UR-REHMAN100% (1)
- Identification From Trace SubstancesDocument52 pagesIdentification From Trace SubstancesARIF-UR-REHMANNo ratings yet
- Firearm InjuriesDocument90 pagesFirearm InjuriesARIF-UR-REHMAN100% (7)
- AsphyxiaDocument48 pagesAsphyxiaARIF-UR-REHMAN100% (1)
- Drug AbuseDocument38 pagesDrug AbuseARIF-UR-REHMAN100% (4)
- Common Poisons 20Document49 pagesCommon Poisons 20ARIF-UR-REHMANNo ratings yet
- Forensic MedicineDocument109 pagesForensic MedicineARIF-UR-REHMAN100% (11)
- 08 Sexual OffencesDocument56 pages08 Sexual OffencesARIF-UR-REHMAN100% (1)
- 04 PutrefactionDocument27 pages04 PutrefactionARIF-UR-REHMAN100% (2)
- 01 Forensic MedicineDocument59 pages01 Forensic MedicineARIF-UR-REHMAN80% (5)
- 3.mechanical InjuryDocument127 pages3.mechanical InjuryARIF-UR-REHMAN100% (2)
- 07 Post Mortem Examination (Autopsy)Document48 pages07 Post Mortem Examination (Autopsy)ARIF-UR-REHMAN100% (5)
- 03 Sudden Death From Natural CauseDocument33 pages03 Sudden Death From Natural CauseARIF-UR-REHMAN100% (2)
- Precision Ground 7075 Aluminum SheetDocument3 pagesPrecision Ground 7075 Aluminum SheetHassan HelmyNo ratings yet
- Bio Lab Report 2Document7 pagesBio Lab Report 2nur ruqayyah74% (19)
- 〈11〉 USP REFERENCE STANDARDS PDFDocument3 pages〈11〉 USP REFERENCE STANDARDS PDFCarlos Fabricio Mendoza AscencioNo ratings yet
- HFC-236FA Extinguisher Data SheetDocument2 pagesHFC-236FA Extinguisher Data SheetRoxanne OquendoNo ratings yet
- Practical 1: Determination of Reducing Sugar Using The Dinitrosalicyclic (DNS) Colourimetric MethodDocument12 pagesPractical 1: Determination of Reducing Sugar Using The Dinitrosalicyclic (DNS) Colourimetric MethodnajwaNo ratings yet
- CSST-10X Hazcom GuideDocument74 pagesCSST-10X Hazcom GuideLuis Rafanan AbiogNo ratings yet
- Pulp paper processesDocument4 pagesPulp paper processesKirana Wirr's50% (2)
- NucleusDocument5 pagesNucleussiddharthr954No ratings yet
- Cromatografía de Capa FinaDocument9 pagesCromatografía de Capa Finadaniela cárdenasNo ratings yet
- Fael Yes Show 425Document9 pagesFael Yes Show 425Ahmed KuttyNo ratings yet
- DAVAO DOCTORS COLLEGE MEDICAL LABORATORY SCIENCE STUDENT NOTES ON BIOCHEMICAL ENERGY PRODUCTIONDocument5 pagesDAVAO DOCTORS COLLEGE MEDICAL LABORATORY SCIENCE STUDENT NOTES ON BIOCHEMICAL ENERGY PRODUCTIONsilvestre bolosNo ratings yet
- The complete guide to get started with injection moldingDocument38 pagesThe complete guide to get started with injection moldingShahadatuliskandar RosliNo ratings yet
- Lakshya Jee 2023: SolutionDocument4 pagesLakshya Jee 2023: SolutionHarshit ChaudharyNo ratings yet
- Earth and Life Science Week 1Document11 pagesEarth and Life Science Week 1raelle tsuNo ratings yet
- Kelvinator KD12MM1 DishwasherDocument24 pagesKelvinator KD12MM1 DishwasherkarlNo ratings yet
- Separate mixtures through distillation and chromatographyDocument2 pagesSeparate mixtures through distillation and chromatographyakshyta gantanNo ratings yet
- Cobalt (II) PhosphateDocument3 pagesCobalt (II) Phosphateengineer bilalNo ratings yet
- Chlorhexidine Stabilizes The Adhesive Interface: A 2-Year inDocument6 pagesChlorhexidine Stabilizes The Adhesive Interface: A 2-Year inAli Al-QaysiNo ratings yet
- PRACTICE WORKSHEET Class 9Document4 pagesPRACTICE WORKSHEET Class 9Atharva VarshneyNo ratings yet
- MSC 2022 Geology Field Report-032023Document42 pagesMSC 2022 Geology Field Report-032023Anurag TopnoNo ratings yet
- Setal D RD 181 X: Technical Data SheetDocument1 pageSetal D RD 181 X: Technical Data SheetさいとはちこNo ratings yet
- Cranberry Evolve+Spec+SheetDocument1 pageCranberry Evolve+Spec+SheetAlmaz KudratovNo ratings yet
- Inorganic Chemistry: An Indian Journal: Pre and Post Compression Studies of TabletsDocument10 pagesInorganic Chemistry: An Indian Journal: Pre and Post Compression Studies of TabletsAugustus OswinNo ratings yet
- SiliconeSealantandStructAdhesives IJAA 2001-21-411Document13 pagesSiliconeSealantandStructAdhesives IJAA 2001-21-411A100% (1)
- Sponge Iron EndorsementDocument17 pagesSponge Iron EndorsementmokeNo ratings yet
- Centrifugal Pumps: What Is A Centrifugal Pump?Document10 pagesCentrifugal Pumps: What Is A Centrifugal Pump?kenoly123No ratings yet
- IB Biology SL - 2024 Prediction Exam - May 2024 Paper 1Document16 pagesIB Biology SL - 2024 Prediction Exam - May 2024 Paper 1Christy HuynhNo ratings yet
- Coconut Grinder Project ReportDocument16 pagesCoconut Grinder Project ReportAli Javed0% (1)
- Influence of Platinum On Mordenite Properties and Catalytic Activity Towards Cyclohexene EpoxidationDocument12 pagesInfluence of Platinum On Mordenite Properties and Catalytic Activity Towards Cyclohexene Epoxidationbruno barrosNo ratings yet
- Biodiesel Production from Sesame Oil and Effect on Diesel Engine PerformanceDocument11 pagesBiodiesel Production from Sesame Oil and Effect on Diesel Engine PerformanceElisabeth NindiNo ratings yet