You might also like
- Andre Tan Updated (With Page Number)Document257 pagesAndre Tan Updated (With Page Number)fiansis100% (2)
- Negative: What Does It Mean To Have A Test Result?Document2 pagesNegative: What Does It Mean To Have A Test Result?Todd EddyNo ratings yet
- Surgery Viva QuestionsDocument24 pagesSurgery Viva QuestionsKay Bristol90% (10)
- Mrcs NotesDocument24 pagesMrcs Notesnob2011nob67% (3)
- 3rd Quarter Examination in Hope 4Document5 pages3rd Quarter Examination in Hope 4Hazel Joan Tan100% (3)
- MCQ MRCSDocument181 pagesMCQ MRCSAmr Sameer100% (15)
- SBA - Anatomy PDFDocument408 pagesSBA - Anatomy PDFabdisamed0% (1)
- Multiple Choice Questions in Paediatric SurgeryFrom EverandMultiple Choice Questions in Paediatric SurgeryRating: 1 out of 5 stars1/5 (1)
- Mrcs VivaDocument573 pagesMrcs VivaAmine Younis93% (15)
- Short Cases in SurgeryDocument115 pagesShort Cases in Surgerynit524100% (2)
- Surgery OSCEDocument23 pagesSurgery OSCEsumith_gunawardhana100% (8)
- Feasibility Study - Spa ResortDocument110 pagesFeasibility Study - Spa ResortMenchie Ella Diezmos Guno100% (2)
- Cyclo ThermDocument24 pagesCyclo ThermProtantagonist91% (11)
- Surgical MCQDocument27 pagesSurgical MCQAhmad Alnemare100% (11)
- Textbook of SurgeryFrom EverandTextbook of SurgeryJoe TjandraNo ratings yet
- Surgery OSCE QuestionsDocument0 pagesSurgery OSCE QuestionsSinginiD86% (7)
- Puzzles in General Surgery: A Study GuideFrom EverandPuzzles in General Surgery: A Study GuideRating: 4.5 out of 5 stars4.5/5 (5)
- 300 Essential SBAs in SurgeryDocument43 pages300 Essential SBAs in SurgeryRicardo Uzcategui ArreguiNo ratings yet
- Surgery MrcsDocument339 pagesSurgery Mrcsdr_shafiq80% (10)
- Man Against HimselfDocument507 pagesMan Against Himselfalbatros3000No ratings yet
- Essential Examination, third edition: Step-by-step guides to clinical examination scenarios with practical tips and key facts for OSCEsFrom EverandEssential Examination, third edition: Step-by-step guides to clinical examination scenarios with practical tips and key facts for OSCEsRating: 3 out of 5 stars3/5 (5)
- Gaps ProtocolDocument3 pagesGaps ProtocolVíctor Valdez100% (2)
- Pass The MRCS PDFDocument533 pagesPass The MRCS PDFYahya Alborno100% (4)
- Clinical Cases and Osces in SurgeryDocument278 pagesClinical Cases and Osces in SurgeryTristan Greene100% (5)
- MRCS Essential ListDocument18 pagesMRCS Essential ListMahmoud Selim100% (1)
- Foundation Skills in Surgery: HandbookFrom EverandFoundation Skills in Surgery: HandbookRating: 3 out of 5 stars3/5 (5)
- MRCS NotesDocument672 pagesMRCS Notessuggaplum100% (6)
- Snippets in Surgery Vol 1: Illustrated Essentials of General SurgeryFrom EverandSnippets in Surgery Vol 1: Illustrated Essentials of General SurgeryRating: 5 out of 5 stars5/5 (1)
- Common Questions Asked in The MRCS Viva Examination PDFDocument4 pagesCommon Questions Asked in The MRCS Viva Examination PDFWael Shoabe100% (1)
- 800 +MCQs-ONLY SUCCESS MRCS-A (UPDATED)Document378 pages800 +MCQs-ONLY SUCCESS MRCS-A (UPDATED)DrTawfik Shabaka100% (1)
- MRCS Clinical 3 1Document47 pagesMRCS Clinical 3 1Alexandros Megas100% (1)
- Critical Care Total MRCS Part BDocument21 pagesCritical Care Total MRCS Part BSnehanshNo ratings yet
- Mrcs Part B Anatomy Stations 11 16 Compilation With Solution 2022Document68 pagesMrcs Part B Anatomy Stations 11 16 Compilation With Solution 2022Pritam RoyNo ratings yet
- Dast20 PDFDocument3 pagesDast20 PDFMarchnuelNo ratings yet
- How To Pass The MRCS PresentationDocument27 pagesHow To Pass The MRCS PresentationKartik sridhar50% (2)
- MRCS B VivaDocument8 pagesMRCS B Vivatahir_the_great2939No ratings yet
- Surgical Career in Uk: Ms Noshin SaiyaraDocument12 pagesSurgical Career in Uk: Ms Noshin SaiyaraMdRimonNo ratings yet
- OSCE Surgery BlockDocument31 pagesOSCE Surgery Blockmyat25100% (6)
- Mind, Society and Behavior - World BankDocument236 pagesMind, Society and Behavior - World BankAnt Green100% (1)
- OSCE Surgery LatestDocument97 pagesOSCE Surgery LatestPrasad Hewawasam0% (1)
- Ge Lightspeed 16 Brochure PDFDocument8 pagesGe Lightspeed 16 Brochure PDFJairo ManzanedaNo ratings yet
- 2 5249132183892787532Document130 pages2 5249132183892787532Asni Longa100% (1)
- Communication Skills MRCSDocument37 pagesCommunication Skills MRCSAnirban Ghosh50% (2)
- MRCS1 2brochureDocument12 pagesMRCS1 2brochuredrsamn100% (2)
- MRCS Book 1 PDFDocument23 pagesMRCS Book 1 PDFAdaad Ahmad67% (6)
- MRCS StationsDocument6 pagesMRCS StationsAnirban Ghosh0% (1)
- Viva For MrcsDocument6 pagesViva For MrcsHasan EljaishNo ratings yet
- General Surgery Board-Final Written Exam Blueprint v.1Document3 pagesGeneral Surgery Board-Final Written Exam Blueprint v.1Mohammed S. Al GhamdiNo ratings yet
- Surgery OsceDocument69 pagesSurgery OsceRebecca BrandonNo ratings yet
- Surgery QuestionsDocument312 pagesSurgery Questionsmonaliza7100% (9)
- A Handbook of Operative Surgery and Surgical Anatomy: With Chapters on InstrumentsFrom EverandA Handbook of Operative Surgery and Surgical Anatomy: With Chapters on InstrumentsRating: 4 out of 5 stars4/5 (5)
- A Guide To MRCS Part BDocument7 pagesA Guide To MRCS Part BWilson Ong Ying FaNo ratings yet
- Pass The MRCS HistoryDocument115 pagesPass The MRCS HistoryMariajanNo ratings yet
- Surgery OSCE PDFDocument26 pagesSurgery OSCE PDFWisal Merghani100% (4)
- The Surgical Portfolio and Interview: A complete guide to preparing for your CST and ST1/ST3From EverandThe Surgical Portfolio and Interview: A complete guide to preparing for your CST and ST1/ST3No ratings yet
- Mrcs Part1Document160 pagesMrcs Part1umaryousuf100% (2)
- Mrcs Viva PDFDocument573 pagesMrcs Viva PDFMaal DaiNo ratings yet
- Service Manual Anestesia Machine GE9100cDocument241 pagesService Manual Anestesia Machine GE9100cYesid Dayan De Leon Escorcia100% (1)
- Intelligent Systems and Technologies in Rehabilitation EngineeringDocument493 pagesIntelligent Systems and Technologies in Rehabilitation EngineeringDorin Triff100% (3)
- Lecture Notes: General Surgery, with Wiley E-TextFrom EverandLecture Notes: General Surgery, with Wiley E-TextRating: 3.5 out of 5 stars3.5/5 (4)
- Surg Osce SummaryDocument7 pagesSurg Osce SummaryShatha AlgahtaniNo ratings yet
- Nta Review of The Effectiveness of Treatment For Alcohol Problems Fullreport 2006 Alcohol2Document212 pagesNta Review of The Effectiveness of Treatment For Alcohol Problems Fullreport 2006 Alcohol2netradeepNo ratings yet
- Manwath Multi-Speciality Hospital: Date of Admission:-Name: - Reg. Bed: DiagnosisDocument1 pageManwath Multi-Speciality Hospital: Date of Admission:-Name: - Reg. Bed: DiagnosisnetradeepNo ratings yet
- The Bile Duct Anastomosis in Liver Transplantation PDFDocument5 pagesThe Bile Duct Anastomosis in Liver Transplantation PDFnetradeepNo ratings yet
- New Microsoft Office PowerPoint PresentationDocument1 pageNew Microsoft Office PowerPoint PresentationnetradeepNo ratings yet
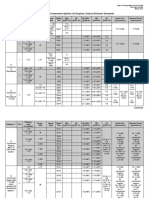
- When To Use What Test PDFDocument8 pagesWhen To Use What Test PDFnetradeepNo ratings yet
- Arrhythmogenic Right Ventricular Cardiomyopathy-CSANZ PDFDocument6 pagesArrhythmogenic Right Ventricular Cardiomyopathy-CSANZ PDFnetradeepNo ratings yet
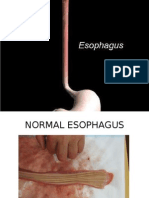
- EsophagusDocument100 pagesEsophagusdr_asrNo ratings yet
- Clinical Conditions Associated With Development of Acute Respiratory Distress SyndromeDocument1 pageClinical Conditions Associated With Development of Acute Respiratory Distress SyndromenetradeepNo ratings yet
- Metabolic SyDocument3 pagesMetabolic SynetradeepNo ratings yet
- Ent DNB DVD TopicsDocument11 pagesEnt DNB DVD TopicsnikitamkNo ratings yet
- Carcinoid Syndrome Crisis and Precipitating PDFDocument32 pagesCarcinoid Syndrome Crisis and Precipitating PDFnetradeepNo ratings yet
- Ca PenisDocument7 pagesCa PenisnetradeepNo ratings yet
- Ca PenisDocument7 pagesCa PenisnetradeepNo ratings yet
- AntidoteDocument5 pagesAntidotenetradeepNo ratings yet
- FistulaDocument23 pagesFistulanetradeep50% (2)
- Jab Tak Ham JiyengeDocument3 pagesJab Tak Ham JiyengenetradeepNo ratings yet
- Shield Intern SheetDocument1 pageShield Intern SheetnetradeepNo ratings yet
- Bankruptcy Restructuring in IndiaDocument16 pagesBankruptcy Restructuring in IndianetradeepNo ratings yet
- For AtdDocument1 pageFor AtdnetradeepNo ratings yet
- A Case Presentation: Under Guidance ofDocument13 pagesA Case Presentation: Under Guidance ofnetradeepNo ratings yet
- 4 Min NeurologicalDocument26 pages4 Min NeurologicalnetradeepNo ratings yet
- GS 3Document44 pagesGS 3netradeepNo ratings yet
- Post-Exposure Prophylaxis For Hiv: CDC GuidelinesDocument26 pagesPost-Exposure Prophylaxis For Hiv: CDC GuidelinesnetradeepNo ratings yet
- Hirschsprung's DsDocument12 pagesHirschsprung's DsnetradeepNo ratings yet
- Critical Care Nursing Clinics of North America Safe Patient Handling 2007Document119 pagesCritical Care Nursing Clinics of North America Safe Patient Handling 2007netradeepNo ratings yet
- Case Presentation Dept. of Medicine VHLDocument13 pagesCase Presentation Dept. of Medicine VHLnetradeepNo ratings yet
- Lower Gi BleedDocument29 pagesLower Gi BleednetradeepNo ratings yet
- Antihypertensive AgentsDocument17 pagesAntihypertensive AgentsGunjan KalyaniNo ratings yet
- Juvenile Justice Act 2015 8460163.ppsxDocument20 pagesJuvenile Justice Act 2015 8460163.ppsxKiran KumarNo ratings yet
- Acupuntura y Tui Na en DismenorreaDocument3 pagesAcupuntura y Tui Na en DismenorreaCristian Dionisio Barros OsorioNo ratings yet
- Soal Tes 1 Sem 6 S1 Reg 2021Document3 pagesSoal Tes 1 Sem 6 S1 Reg 2021arka jrNo ratings yet
- Quality Assurance 608Document42 pagesQuality Assurance 608ENTREPRENEUR 8211No ratings yet
- T&C Procedure Grease Interceptors Vida Ok 13sept2020Document115 pagesT&C Procedure Grease Interceptors Vida Ok 13sept2020Gopa KumarNo ratings yet
- The IASP Classification of Chronic Pain For.10Document6 pagesThe IASP Classification of Chronic Pain For.10hzol83No ratings yet
- Hand Injuries & Their ManagementsDocument78 pagesHand Injuries & Their ManagementsKuruNo ratings yet
- Robots in Shipbuilding Industry (1160) PDFDocument9 pagesRobots in Shipbuilding Industry (1160) PDFWahyu WahyurachmatdhaniNo ratings yet
- EPA Emission StandardsDocument5 pagesEPA Emission StandardsSyed Zain AhmadNo ratings yet
- NIOS Sec PsychologyDocument383 pagesNIOS Sec PsychologySujitha DhanarajNo ratings yet
- Factual ReportDocument5 pagesFactual Report13Ni Putu Eka MartiniNo ratings yet
- VAL-SV-E0163-P PCBA Depanelization Router Elite Machine Validation Plan - Edy-29 Nov (CK)Document8 pagesVAL-SV-E0163-P PCBA Depanelization Router Elite Machine Validation Plan - Edy-29 Nov (CK)arumNo ratings yet
- Allison H. Feibus, MD, MS: Summa Cum LaudeDocument9 pagesAllison H. Feibus, MD, MS: Summa Cum Laudemmmmder7No ratings yet
- Avoiding The Line of Fire: "For Safety's Sake - Do Something"Document1 pageAvoiding The Line of Fire: "For Safety's Sake - Do Something"Sergio SáezNo ratings yet
- Catalog DAIKIN 2013 SingDocument47 pagesCatalog DAIKIN 2013 SingVan Diep100% (1)
- Mr. Abhishek Bajpai Bajpai: Wellwise Advanced ProfileDocument40 pagesMr. Abhishek Bajpai Bajpai: Wellwise Advanced ProfileAbhishek BajpaiNo ratings yet
- Cierre Percutaneo de Pca en PrematurosDocument12 pagesCierre Percutaneo de Pca en PrematurosNancy Romero QuirosNo ratings yet
- Language Development: - Iphy OkoyeDocument9 pagesLanguage Development: - Iphy OkoyeIPHY OKOYENo ratings yet