You might also like
- Bronchial Asthma in Acute Exacerbation - FinalDocument17 pagesBronchial Asthma in Acute Exacerbation - Finalmary_sulit_150% (2)
- Case Study On AsthmaDocument21 pagesCase Study On AsthmaJerome Vergara75% (4)
- Understanding Bronchial AsthmaDocument25 pagesUnderstanding Bronchial AsthmaRio Jane AsimanNo ratings yet
- Case Study (Bronchial Asthma)Document11 pagesCase Study (Bronchial Asthma)DhanNie Cenita50% (2)
- Asthma (Case Study 6)Document14 pagesAsthma (Case Study 6)Mylz MendozaNo ratings yet
- Case Analysis Bronchial AsthmaDocument21 pagesCase Analysis Bronchial AsthmaKim LladaNo ratings yet
- Case Study of Bronchial Asthma in Acute ExacerbationDocument16 pagesCase Study of Bronchial Asthma in Acute Exacerbationdextroid1290% (29)
- ER Treatment for Asthmatic PatientDocument4 pagesER Treatment for Asthmatic PatientEver Green100% (2)
- BRONCHIAL ASTHMA Case Presentation. EditedDocument37 pagesBRONCHIAL ASTHMA Case Presentation. Edited92006770% (10)
- CASE STUDY Bronchial AsthmaDocument6 pagesCASE STUDY Bronchial AsthmaRichelle Sandriel C. de Castro86% (22)
- Case Study On AsthmaDocument17 pagesCase Study On Asthmaremybutalid100% (2)
- Case Study of Bronchial Asthma in Acute ExacerbationDocument19 pagesCase Study of Bronchial Asthma in Acute ExacerbationEzra Dizon ManzanoNo ratings yet
- Bronchial Asthma I. Objectives: A. U: - Espiratory InfectionsáDocument5 pagesBronchial Asthma I. Objectives: A. U: - Espiratory InfectionsáEnah EvangelistaNo ratings yet
- A Case Study On Bronchial Asthma in Acute ExacerbationDocument71 pagesA Case Study On Bronchial Asthma in Acute ExacerbationATEHAN BORDSNo ratings yet
- Bronchial Asthma: A Case PresentationDocument59 pagesBronchial Asthma: A Case Presentationjava_biscocho122985% (39)
- Case Study On Bronchial AsthmaDocument29 pagesCase Study On Bronchial Asthmamanny valenciaNo ratings yet
- Bronchial Asthma in AEDocument14 pagesBronchial Asthma in AECharmie Lou Dadivas CelestialNo ratings yet
- Case Study On AsthmaDocument8 pagesCase Study On AsthmaDoff Cruz100% (1)
- Understanding Pneumonia PathophysiologyDocument3 pagesUnderstanding Pneumonia PathophysiologyKaloy KamaoNo ratings yet
- Asthma!!!Document18 pagesAsthma!!!Jabbamackeez50% (2)
- Bronchial AsthmaDocument29 pagesBronchial AsthmaDrShaheen100% (5)
- Asthma - Case PresentationDocument56 pagesAsthma - Case Presentationsarooah199467% (6)
- I Can'T Breathe If Breathing Is Without: Bronchial AsthmaDocument33 pagesI Can'T Breathe If Breathing Is Without: Bronchial AsthmaklamorenaNo ratings yet
- Case Summary of Patient With Chronic Obstructive PulmonaryDocument27 pagesCase Summary of Patient With Chronic Obstructive PulmonaryUzair Muhd0% (1)
- Pediatric Asthma PDFDocument12 pagesPediatric Asthma PDFzie_luph_taz13No ratings yet
- PneumoniaDocument17 pagesPneumoniajustin_saneNo ratings yet
- Acute Bronchitis Case StudyDocument6 pagesAcute Bronchitis Case Studyulka0750% (2)
- Case Study (Asthma)Document3 pagesCase Study (Asthma)AIM50% (4)
- COPD Case PresentationDocument50 pagesCOPD Case PresentationSarah Ann Jamilla FaciolanNo ratings yet
- Bronchial AsthmaDocument8 pagesBronchial AsthmaBrylle CapiliNo ratings yet
- Bronchial Asthma (Case Study)Document12 pagesBronchial Asthma (Case Study)Adriane Coma100% (1)
- Case Study - PneumoniaDocument41 pagesCase Study - PneumoniaCaleb Mcmahon67% (6)
- Case Study of BronchoPneumoniaDocument64 pagesCase Study of BronchoPneumoniaJomari Zapanta100% (2)
- Meconium Aspiration Syndrome: Causes, Symptoms and TreatmentDocument38 pagesMeconium Aspiration Syndrome: Causes, Symptoms and TreatmentGrace Antonette Pati100% (1)
- Pneumonia: Causes, Signs, Symptoms and Nursing CareDocument16 pagesPneumonia: Causes, Signs, Symptoms and Nursing CareMelissa David100% (1)
- Drug Study Lab, NCP - Bronchial AsthmaDocument6 pagesDrug Study Lab, NCP - Bronchial AsthmaRichelle Sandriel C. de CastroNo ratings yet
- Bronchial Asthma in Acute Exacerbation Case StudyDocument43 pagesBronchial Asthma in Acute Exacerbation Case Studyroseanne parkNo ratings yet
- Pneumonia Case StudyDocument24 pagesPneumonia Case StudyDharylle Cariño100% (1)
- Pneumonia Case PresentationDocument24 pagesPneumonia Case Presentationudanics100% (1)
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- Case Study PneumoniaDocument17 pagesCase Study Pneumoniajhilltot100% (2)
- Asthma Case Study: 11-Year-Old Boy with Breathing DifficultyDocument23 pagesAsthma Case Study: 11-Year-Old Boy with Breathing DifficultyBHARTI SINGH92% (13)
- Tetralogy of Fallot Nursing CaseDocument32 pagesTetralogy of Fallot Nursing CaseUday Kumar50% (2)
- Rheumatic Heart DiseaseDocument8 pagesRheumatic Heart DiseaseJehannaMarEnggingAbdurahmanNo ratings yet
- A Case Study On PnuemoniaDocument23 pagesA Case Study On Pnuemoniaxyzert88% (8)
- Nursing Care of Bronchial AsthmaDocument16 pagesNursing Care of Bronchial AsthmaIntan RahmiNo ratings yet
- Case Study Pneumonia)Document20 pagesCase Study Pneumonia)Jai - Ho83% (6)
- !M !M !M !M !M !M !MDocument5 pages!M !M !M !M !M !M !MJazie Pitpitunge BognadonNo ratings yet
- Nursing Interventions: Asthma: PathoDocument4 pagesNursing Interventions: Asthma: Pathomische20No ratings yet
- File 18585Document15 pagesFile 18585Mohammed MuthanaNo ratings yet
- Case Presentation GeriatricDocument35 pagesCase Presentation GeriatricNurdina AfiniNo ratings yet
- Bronchial AsthmaDocument95 pagesBronchial AsthmaBrian BrownNo ratings yet
- ASTHMADocument9 pagesASTHMAHamza DibNo ratings yet
- Vestil - Case Study On AsthmaDocument7 pagesVestil - Case Study On Asthmaninachristenevestil25No ratings yet
- Respiratory Disorder Note BSC 3rd YearDocument41 pagesRespiratory Disorder Note BSC 3rd YearNancyNo ratings yet
- CHD AsthmaDocument20 pagesCHD AsthmaRj MagpayoNo ratings yet
- AsthmaDocument9 pagesAsthmaNiña Jemia CortezNo ratings yet
- Bronchial AsthmaDocument54 pagesBronchial AsthmaSehar162100% (2)
- Asthma Davidson + Osmosis + Step Up MedicineDocument2 pagesAsthma Davidson + Osmosis + Step Up MedicineElyas MehdarNo ratings yet
- Asthma: Kinyua Md. MCM - A & E MKU Facilitator: Dr. AyungaDocument28 pagesAsthma: Kinyua Md. MCM - A & E MKU Facilitator: Dr. AyungaDennis MiritiNo ratings yet
- RespiratoryDocument249 pagesRespiratorybuzz Q100% (3)
- Case Study of LeptospirosisDocument4 pagesCase Study of Leptospirosisbuzz Q75% (4)
- Case Study of DMDocument6 pagesCase Study of DMbuzz Q0% (1)
- Case Study of Liver CirrhosisDocument3 pagesCase Study of Liver Cirrhosisbuzz Q100% (1)
- Case Study of AmoebiasisDocument7 pagesCase Study of Amoebiasisbuzz Q75% (4)
- GUT3Document143 pagesGUT3buzz Q100% (1)
- ReadmeDocument1 pageReadmebuzz QNo ratings yet
- Musical InstrumentsDocument12 pagesMusical Instrumentsbuzz QNo ratings yet
- Phobia ListDocument48 pagesPhobia Listbuzz QNo ratings yet
- Growth and DevelopmentDocument6 pagesGrowth and Developmentbuzz Q100% (3)
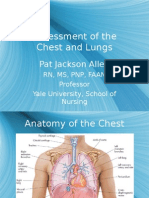
- Assessment of The Chest and Lungs: Pat Jackson AllenDocument50 pagesAssessment of The Chest and Lungs: Pat Jackson Allenbuzz Q100% (3)
- Assessment Slide ShowDocument144 pagesAssessment Slide Showbuzz QNo ratings yet
- AbdomenDocument100 pagesAbdomenbuzz Q83% (6)
- Assessment of The Skin: Pat Jackson AllenDocument104 pagesAssessment of The Skin: Pat Jackson Allenbuzz Q100% (4)
- Care of The NewbornDocument5 pagesCare of The Newbornbuzz Q100% (2)
- CardiovascularDocument122 pagesCardiovascularbuzz QNo ratings yet
- UrologyDocument28 pagesUrologybuzz QNo ratings yet
- ImmunologyDocument23 pagesImmunologybuzz QNo ratings yet
- The Reproductive SystemDocument18 pagesThe Reproductive Systembuzz QNo ratings yet
- The Cardiovascular SystemDocument20 pagesThe Cardiovascular Systembuzz QNo ratings yet
- SensesDocument44 pagesSensesbuzz Q100% (1)
- The Pulmonary SystemDocument21 pagesThe Pulmonary Systembuzz QNo ratings yet
- Digestive SystemDocument38 pagesDigestive Systembuzz QNo ratings yet
- NeurologyDocument42 pagesNeurologybuzz Q100% (2)
- Musculoskeletal SystemDocument50 pagesMusculoskeletal Systembuzz QNo ratings yet
- Basic ChemistryDocument47 pagesBasic Chemistrybuzz QNo ratings yet
- DermaDocument33 pagesDermabuzz QNo ratings yet
- The Anaerobic Threshold 50 Years of ControversyDocument31 pagesThe Anaerobic Threshold 50 Years of ControversyHansCristopherSaegerPizarroNo ratings yet
- Nursing Process Guide: St. Anthony's College Nursing DepartmentDocument10 pagesNursing Process Guide: St. Anthony's College Nursing DepartmentAngie MandeoyaNo ratings yet
- CARESCAPE R860 Ventilator Clinical Accessories Guide - JB79010XXDocument16 pagesCARESCAPE R860 Ventilator Clinical Accessories Guide - JB79010XXelcio_sousaNo ratings yet
- AIR QUALITY AND POLLUTION (TKA 3301) LECTURE NOTES 4-Chemistry of Air Pollution N Ideal Gas LawDocument66 pagesAIR QUALITY AND POLLUTION (TKA 3301) LECTURE NOTES 4-Chemistry of Air Pollution N Ideal Gas Lawmamat88No ratings yet
- Art and Creativity Meditation TechniquesDocument2 pagesArt and Creativity Meditation TechniquesLivgian KaurNo ratings yet
- Blish, James - Surface TensionDocument45 pagesBlish, James - Surface TensionFuzzyyyy100% (4)
- Lalana Newborn ResuscitationDocument55 pagesLalana Newborn ResuscitationAthenaeum Scientific PublishersNo ratings yet
- Wellness Massage 9-Q2-Module 4Document27 pagesWellness Massage 9-Q2-Module 4Kim Caguioa67% (3)
- Blue and Purple Mental Health Modern User Information BrochureDocument1 pageBlue and Purple Mental Health Modern User Information BrochureJohn Carl B. BungarNo ratings yet
- Personal Power II Flash CardsDocument41 pagesPersonal Power II Flash CardsDonald Mok100% (9)
- Safety Data SheetsDocument150 pagesSafety Data SheetsHitesh Soni0% (1)
- Understanding Merkaba MechanicsDocument19 pagesUnderstanding Merkaba MechanicsKazi Riasat Alve100% (1)
- PTB NCPDocument3 pagesPTB NCPناديه المعمريNo ratings yet
- 07 IfU Savina 300 SW 5 N enDocument274 pages07 IfU Savina 300 SW 5 N enBernardo CostaNo ratings yet
- April e Mag of TWUYADocument21 pagesApril e Mag of TWUYAAshish Mahajan100% (1)
- 1 - Fundamentals of Speech CommunicationDocument12 pages1 - Fundamentals of Speech CommunicationInga Budadoy NaudadongNo ratings yet
- The Role of the Diaphragm in BreathingDocument2 pagesThe Role of the Diaphragm in BreathingLynda BarrowNo ratings yet
- Feeding Your Demons Tsultrim AllioneDocument9 pagesFeeding Your Demons Tsultrim Allionethe tri namNo ratings yet
- Week 5-Earth-and-Life-ScienceDocument80 pagesWeek 5-Earth-and-Life-ScienceChaeyoung ParkNo ratings yet
- General lab instructions and experimentsDocument17 pagesGeneral lab instructions and experimentsErica De Guzman100% (1)
- Life Support Test Facility LSTF100Document3 pagesLife Support Test Facility LSTF100Bojana MarinkovicNo ratings yet
- Chapter Eight - Maintaining Technique Under PressureDocument15 pagesChapter Eight - Maintaining Technique Under PressureAus Al-majmueiNo ratings yet
- Richard Lowell Hittleman - Richard Hittleman's Yoga - 28 Day Exercise Plan (1973 (1969), Bantam Books)Document324 pagesRichard Lowell Hittleman - Richard Hittleman's Yoga - 28 Day Exercise Plan (1973 (1969), Bantam Books)Laissi AbdallahNo ratings yet
- Due: Submitted On or Before Sunday September 11 at 11:59 PM With No PenaltyDocument2 pagesDue: Submitted On or Before Sunday September 11 at 11:59 PM With No PenaltyVictor KulobaNo ratings yet
- IGCSE Biology Bullet PointsDocument34 pagesIGCSE Biology Bullet PointslordeNo ratings yet
- Final Poly 2.aDocument19 pagesFinal Poly 2.akimberlyn odoñoNo ratings yet
- The American Union Speaker by Philbrick, John D.Document410 pagesThe American Union Speaker by Philbrick, John D.Gutenberg.orgNo ratings yet
- Recommendations For Respiratory Rehabilitation In.99313 PDFDocument26 pagesRecommendations For Respiratory Rehabilitation In.99313 PDFLeandro VillamilNo ratings yet
- RPT SC Form 1Document22 pagesRPT SC Form 1Norhidayah Binti PazilNo ratings yet
- Breath Holding TimesDocument28 pagesBreath Holding TimesReina RamirezNo ratings yet