You might also like
- Pulmonary ThromboembolismDocument61 pagesPulmonary ThromboembolismsanjivdasNo ratings yet
- 4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFDocument89 pages4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFjackie funtanilla100% (1)
- C TrialsDocument24 pagesC TrialsFauzi SebunyaNo ratings yet
- Acute Renal FailureDocument9 pagesAcute Renal FailureananNo ratings yet
- Dermatological PharmacologyDocument25 pagesDermatological Pharmacologyborneo225100% (1)
- Final GIT Case PresentationDocument53 pagesFinal GIT Case PresentationRovan100% (1)
- Drug Treatment of AnemiaDocument36 pagesDrug Treatment of Anemiadoctorneha66No ratings yet
- Medication ChartDocument2 pagesMedication Chartmax_21ru100% (1)
- Nursing ATIDocument55 pagesNursing ATINicoleta AndreiNo ratings yet
- Anaesthesia For Patients With COPD: University College of Medical Sciences & GTB Hospital, DelhiDocument76 pagesAnaesthesia For Patients With COPD: University College of Medical Sciences & GTB Hospital, DelhiRINI100% (1)
- Viral Hepatitis PDFDocument4 pagesViral Hepatitis PDFNina BracyNo ratings yet
- Heart DiseaseDocument11 pagesHeart Diseaseapi-529065933No ratings yet
- Kit System ManagementDocument29 pagesKit System ManagementTifa IstiwaNo ratings yet
- Optimized Clinical Case StudiesDocument4 pagesOptimized Clinical Case StudiesAassh DcmbrNo ratings yet
- Anatomy of PancreasDocument2 pagesAnatomy of PancreasAubrey MacNo ratings yet
- Thyroid Gland BasicsDocument25 pagesThyroid Gland BasicsSreekar DevarakondaNo ratings yet
- Anatomy Urinary System GuideDocument5 pagesAnatomy Urinary System GuideJaye DangoNo ratings yet
- Cvs PathoDocument36 pagesCvs PathoISRAELNo ratings yet
- QOch 11 Studyguide QODocument16 pagesQOch 11 Studyguide QOHenry HoNo ratings yet
- ANP Heart Anatomy & PhysiologyDocument3 pagesANP Heart Anatomy & PhysiologySheana Tmpl100% (1)
- Hepatic DisordersDocument15 pagesHepatic DisordersKenneth OpinaNo ratings yet
- Anti EmeticsDocument29 pagesAnti EmeticsBezawit Tsige100% (1)
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuNo ratings yet
- Preoperative Assessment ChecklistDocument27 pagesPreoperative Assessment ChecklistHairina MazlanNo ratings yet
- Astmul Bronsic: Scoala Sanitara "G. Gh. Voda"-Iasi - Curs Pneumologie, Anul II, Dr. Roxana Radu (Poleac)Document5 pagesAstmul Bronsic: Scoala Sanitara "G. Gh. Voda"-Iasi - Curs Pneumologie, Anul II, Dr. Roxana Radu (Poleac)Postolache IlonaNo ratings yet
- 9149StatlerMentalStatus PDFDocument5 pages9149StatlerMentalStatus PDFArumDesiPratiwiNo ratings yet
- Thyroid HormonesDocument63 pagesThyroid HormonesDr. M. Prasad NaiduNo ratings yet
- Pancreas: - Anatomy and Histology - Normal Physiology of The Endocrine PancreasDocument34 pagesPancreas: - Anatomy and Histology - Normal Physiology of The Endocrine PancreasironNo ratings yet
- Acute Coronary Syndrome GuideDocument57 pagesAcute Coronary Syndrome Guideendah100% (1)
- Approach To Comatose Child: DR G.VenkateshDocument83 pagesApproach To Comatose Child: DR G.VenkateshG VenkateshNo ratings yet
- Tocolytic Agents and Anticonvulsants for Preterm LabourDocument95 pagesTocolytic Agents and Anticonvulsants for Preterm LabourPriya jNo ratings yet
- Blood Gas MachineDocument33 pagesBlood Gas MachinenofearnofearNo ratings yet
- Cardio Vascular SystemDocument22 pagesCardio Vascular SystemdeborahNo ratings yet
- Ethiopian National Drug FormularyDocument572 pagesEthiopian National Drug FormularyportosinNo ratings yet
- Clinical Case Diabetes Insipidus-2Document11 pagesClinical Case Diabetes Insipidus-2Marga Koury100% (1)
- GERIATRIC MEDICINE (Basic)Document41 pagesGERIATRIC MEDICINE (Basic)Medical AdvicesNo ratings yet
- Disorders of Endocrine System: Prof. J. Hanáček, MD, PHDDocument66 pagesDisorders of Endocrine System: Prof. J. Hanáček, MD, PHDjerinthomasrajanNo ratings yet
- 2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDDocument58 pages2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDKishan SethNo ratings yet
- Guideline Antibiotic RationalDocument35 pagesGuideline Antibiotic RationalIstianah EsNo ratings yet
- Makalah HypertensionDocument6 pagesMakalah HypertensionFatin ZafirahNo ratings yet
- Depression: Understanding the Leading Mental Health ConditionDocument38 pagesDepression: Understanding the Leading Mental Health Conditiondrmsupriya091159No ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- Evaluation of Chest Pain in Primary Care Patients-AAFPDocument3 pagesEvaluation of Chest Pain in Primary Care Patients-AAFPnouval_iqbalNo ratings yet
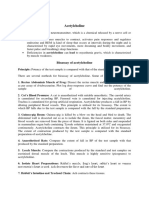
- Acetylcholine Bioassay MethodsDocument1 pageAcetylcholine Bioassay MethodsSangi RajNo ratings yet
- Medicina in ViitorDocument1 pageMedicina in ViitorNicolae CristianNo ratings yet
- Diabesity: A New Paradigm of Metabolic ConnexionDocument37 pagesDiabesity: A New Paradigm of Metabolic ConnexionatezorNo ratings yet
- Autacoids: Group No. 1Document92 pagesAutacoids: Group No. 1Rohan Pal100% (1)
- Renal PharmacologyDocument52 pagesRenal PharmacologyashrafNo ratings yet
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22No ratings yet
- Pharma Rapid Review FOCUSDocument85 pagesPharma Rapid Review FOCUSKeelNo ratings yet
- Pharmacotherapy of PneumoniaDocument56 pagesPharmacotherapy of Pneumoniahoneylemon.co100% (1)
- ARBs (Angiotensin II Receptor Blockers) NCLEXDocument15 pagesARBs (Angiotensin II Receptor Blockers) NCLEXSameerQadumi100% (1)
- Surfactant PresentationDocument18 pagesSurfactant PresentationMaadaNo ratings yet
- COPD ExacerbationDocument2 pagesCOPD ExacerbationjusthoangNo ratings yet
- Clinical Reasoning For Nursing Students - Glossary of TermsDocument22 pagesClinical Reasoning For Nursing Students - Glossary of Termsmillstoneridge1100% (1)
- Antifungal Drugs: - Polyene Antibiotics: Amphotericin B, Nystatin - Antimetabolites: 5-Fluorocytosine - AzolesDocument18 pagesAntifungal Drugs: - Polyene Antibiotics: Amphotericin B, Nystatin - Antimetabolites: 5-Fluorocytosine - AzolesgopscharanNo ratings yet
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocument41 pagesDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityredderdatNo ratings yet
- Clinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978From EverandClinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978P. Duchêne-MarullazNo ratings yet
- SacacascsaDocument1 pageSacacascsaefendiNo ratings yet
- Blank Cause and Effect DiagramDocument1 pageBlank Cause and Effect DiagramefendiNo ratings yet
- Fishbone Diagram Template 27 PDFDocument1 pageFishbone Diagram Template 27 PDFefendiNo ratings yet
- Ahajf HSFHGDocument1 pageAhajf HSFHGefendiNo ratings yet
- Dnkgjhsha GbkjjvbsanknvzkvdalDocument1 pageDnkgjhsha GbkjjvbsanknvzkvdalefendiNo ratings yet
- Pharmacology MCQs 1Document10 pagesPharmacology MCQs 1efendi100% (2)
- IntroductionDocument1 pageIntroductionefendiNo ratings yet
- Guidelines NSTE ACSDocument56 pagesGuidelines NSTE ACSPedro Perez FuentesNo ratings yet
- Medical Faculty Hasanuddin University Makassar 2010: Clinical Pathology Lab Urogenitalia SystemDocument8 pagesMedical Faculty Hasanuddin University Makassar 2010: Clinical Pathology Lab Urogenitalia SystemefendiNo ratings yet
- Anterior Septal Stemi With OnsetDocument32 pagesAnterior Septal Stemi With OnsetefendiNo ratings yet
- Clin Infect Dis.-2010-Solomkin-133-64 (D and M of Complicated Intra-Abdominal Infection in Adults and Children) PDFDocument32 pagesClin Infect Dis.-2010-Solomkin-133-64 (D and M of Complicated Intra-Abdominal Infection in Adults and Children) PDFefendiNo ratings yet
- Report Group 6 Module 4 Scenario 1Document18 pagesReport Group 6 Module 4 Scenario 1efendiNo ratings yet
- Pharyngitis Guide: Etiology, Diagnosis & ManagementDocument21 pagesPharyngitis Guide: Etiology, Diagnosis & ManagementefendiNo ratings yet
- Praktikum UjianDocument46 pagesPraktikum UjianefendiNo ratings yet
- Soal Neuro 5 Desember 2011Document11 pagesSoal Neuro 5 Desember 2011efendiNo ratings yet
- Soal Neuro 5 Desember 2011Document11 pagesSoal Neuro 5 Desember 2011efendiNo ratings yet
- Ekg InterpretareDocument25 pagesEkg InterpretareTeodor SlabuNo ratings yet
- الدكتور مصطفى الشناق رئيس جمعية الجهاز الهضمي والكبد الأردنية Medics Index Member 10122010 ResumeDocument29 pagesالدكتور مصطفى الشناق رئيس جمعية الجهاز الهضمي والكبد الأردنية Medics Index Member 10122010 ResumejordanmedicsNo ratings yet
- Non St-Segment Elevation Acute Coronary Syndrome (Nste-Acs) : EtiologyDocument4 pagesNon St-Segment Elevation Acute Coronary Syndrome (Nste-Acs) : EtiologyKEn PilapilNo ratings yet
- Complications of DialysisDocument7 pagesComplications of DialysisDilessandro PieroNo ratings yet
- 5 Min - Myocardial Strain AnalysisDocument26 pages5 Min - Myocardial Strain AnalysisAsim Kumar Biswas100% (1)
- Test Bank For Building A Medical Vocabulary 7th Edition Leonard DownloadDocument20 pagesTest Bank For Building A Medical Vocabulary 7th Edition Leonard Downloadalidangana683No ratings yet
- ACLS DrugsDocument4 pagesACLS DrugsEduard Espeso Chiong-Gandul Jr.No ratings yet
- Cardioversion & Defibrillation ExplainedDocument18 pagesCardioversion & Defibrillation ExplainedJannah Marie A. Dimaporo100% (4)
- Reading Versola Ventricular TachycardiaDocument3 pagesReading Versola Ventricular TachycardiaRaijenne VersolaNo ratings yet
- Cardiovascular SystemDocument624 pagesCardiovascular Systempattumkp100% (1)
- Doctors OET Writing Practice TestDocument3 pagesDoctors OET Writing Practice Testanjali hansNo ratings yet
- UPDATED - Recruiting NHS Organisations and Contact Details Website - 23-24 - 0Document11 pagesUPDATED - Recruiting NHS Organisations and Contact Details Website - 23-24 - 0Naga MuthuNo ratings yet
- Comparison Study. CARESCAPEB850Document4 pagesComparison Study. CARESCAPEB850Alberto MHNo ratings yet
- ALSDocument35 pagesALSZainal ArifinNo ratings yet
- Arritmias VentricularesDocument11 pagesArritmias VentricularesJesusIsmaelCoronaNo ratings yet
- Philippine Heart Association 42nd Annual Convention GuideDocument7 pagesPhilippine Heart Association 42nd Annual Convention GuideGene Alfonso BanawaNo ratings yet
- Acls Drug OverviewDocument2 pagesAcls Drug OverviewBruce Abramowitz100% (1)
- CardiologyDocument83 pagesCardiologyAshutosh SinghNo ratings yet
- A GLIMPSE Into Cardiology 2022Document48 pagesA GLIMPSE Into Cardiology 2022Ashvanee Kumar SharmaNo ratings yet
- Ischaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeDocument104 pagesIschaemic Heart Disease: DR Haider Baqai Assistant Professor of Medicine Rawalpindi Medical CollegeputriluftiNo ratings yet
- DR - Amit Kumar Chaurasia - Artemis - CardiologyDocument3 pagesDR - Amit Kumar Chaurasia - Artemis - CardiologyAkash RajNo ratings yet
- Coronary Artery DiseaseDocument13 pagesCoronary Artery DiseaseChristianHanjokarNo ratings yet
- (OSCE) 3.0 Cardiovascular ExaminationDocument5 pages(OSCE) 3.0 Cardiovascular ExaminationJara RogacionNo ratings yet
- Altered Tissue PerfusionDocument10 pagesAltered Tissue PerfusionLaurence ZernaNo ratings yet
- CardiomyopathyDocument93 pagesCardiomyopathyAbnet WondimuNo ratings yet
- ECOCARDIODocument3 pagesECOCARDIOArun ComedsNo ratings yet
- Managing nutrition for chronic kidney disease patientsDocument29 pagesManaging nutrition for chronic kidney disease patientsPinny Rilenda L NgaraNo ratings yet
- NCLEX Practice Exam 21 (60 Questions)Document36 pagesNCLEX Practice Exam 21 (60 Questions)Melodia Turqueza GandezaNo ratings yet
- Diagnosis: Imaging of Valvular Heart Disease in Heart FailureDocument9 pagesDiagnosis: Imaging of Valvular Heart Disease in Heart FailureAudini BerbasariNo ratings yet
- RCP Consultant Physicians Working With PatientsDocument266 pagesRCP Consultant Physicians Working With PatientsalaaNo ratings yet