You might also like
- Teen MedicalDocument1 pageTeen MedicalJohn C StarkNo ratings yet
- Vermara Kids Daycare Registration Form 2Document5 pagesVermara Kids Daycare Registration Form 2api-29050616No ratings yet
- Rockford Rec Emergency Medical FormDocument2 pagesRockford Rec Emergency Medical FormRyan ThompsonNo ratings yet
- Please Complete A Form For EACH Student.: Last First Middle InitialDocument4 pagesPlease Complete A Form For EACH Student.: Last First Middle InitialhwienNo ratings yet
- Guest Consent Release Form For Outside Groups Using Young Life CampDocument1 pageGuest Consent Release Form For Outside Groups Using Young Life Campkschwahn1No ratings yet
- ChildenrollmentpapersDocument7 pagesChildenrollmentpapersapi-531837774No ratings yet
- Child's Application: Sample FormDocument3 pagesChild's Application: Sample FormLaura ParkaNo ratings yet
- Emergency Medical FormDocument2 pagesEmergency Medical FormDenisa BobocNo ratings yet
- Clinical Health RequirementsDocument6 pagesClinical Health RequirementsbarneylovesbagelsNo ratings yet
- New Patient Information Form PrintableDocument3 pagesNew Patient Information Form PrintableXyzNo ratings yet
- Sis-Form SLNHSDocument1 pageSis-Form SLNHSMICHAEL RUELONo ratings yet
- ZENITH INTERNATIONAL SCHOOLS Employment FormDocument1 pageZENITH INTERNATIONAL SCHOOLS Employment FormolootukingNo ratings yet
- Student InformationDocument1 pageStudent Informationchantel_allenNo ratings yet
- RX Incident Report FormDocument2 pagesRX Incident Report FormArthur KrichevskyNo ratings yet
- Velocity Health FormDocument2 pagesVelocity Health FormChris HansenNo ratings yet
- Sanlo Applicants Data v.201602 PDFDocument2 pagesSanlo Applicants Data v.201602 PDFVenTenNo ratings yet
- Writable PC FormDocument1 pageWritable PC FormJulie Vyne ModalesNo ratings yet
- 2009 Enrollment FormsDocument2 pages2009 Enrollment FormsesromseanNo ratings yet
- Emergency Medical Information Form: Check All That ApplyDocument3 pagesEmergency Medical Information Form: Check All That Applyamber leighNo ratings yet
- Admin ApplicationDocument3 pagesAdmin ApplicationRedeemer Lutheran SchoolNo ratings yet
- Player Medical Information FormDocument1 pagePlayer Medical Information FormKorey BradleyNo ratings yet
- Adult Health HistoryDocument1 pageAdult Health HistorySally Hansen100% (1)
- Info SheetDocument1 pageInfo SheetShaun Louis AbunyawanNo ratings yet
- Hospital Admission FormDocument1 pageHospital Admission FormAsep SetiawanNo ratings yet
- ApplicationDocument2 pagesApplicationGrace Deleeuw PelusoNo ratings yet
- Axa Mansard Health Corporate Form - Nathan Ayomide OriaifoDocument1 pageAxa Mansard Health Corporate Form - Nathan Ayomide OriaifoIsiNo ratings yet
- WOW Kid's Club Health FormDocument4 pagesWOW Kid's Club Health FormKetron Memorial United Methodist ChurchNo ratings yet
- Notes: Face AmountDocument4 pagesNotes: Face Amountqris24No ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- Rosemont Junior Medical ReleaseDocument1 pageRosemont Junior Medical Releasecorndog1No ratings yet
- Application Form InitialDocument2 pagesApplication Form InitialSaori NagaseNo ratings yet
- Client Personal Information FormDocument3 pagesClient Personal Information FormRD Finders and Personal Training100% (1)
- ApplicationDocument2 pagesApplicationMark McCoyNo ratings yet
- Lincoln-Woodstock Cooperative School District SAU # 68Document4 pagesLincoln-Woodstock Cooperative School District SAU # 68Daniel AdamsNo ratings yet
- 2011 Vbs Registration Rev31 3Document1 page2011 Vbs Registration Rev31 3api-65033158No ratings yet
- FEBC Info Sheet - NEWDocument5 pagesFEBC Info Sheet - NEWnigel alinsug0% (1)
- Information SheetDocument2 pagesInformation SheetimpbarryNo ratings yet
- Print PDFDocument1 pagePrint PDFLatrendaNo ratings yet
- Form R 30 Student Information SheetDocument1 pageForm R 30 Student Information SheetAngelica Diana AquinoNo ratings yet
- Pa Part Waiver 08Document1 pagePa Part Waiver 08vickiecavanagh100% (1)
- Enrollment FormDocument5 pagesEnrollment Formapi-738612218No ratings yet
- Observer Ship ApplicationDocument1 pageObserver Ship ApplicationAgape6672No ratings yet
- History Form For AdultsDocument9 pagesHistory Form For AdultsFazal HaqueNo ratings yet
- Pcs Emergency Permission Form - 21-22Document1 pagePcs Emergency Permission Form - 21-22api-671085061No ratings yet
- Staff Physician's Report 2016Document4 pagesStaff Physician's Report 2016Anonymous zzXPtsgNo ratings yet
- Medical FormDocument1 pageMedical Formapi-144496227No ratings yet
- ApplicationDocument3 pagesApplicationapi-107554386No ratings yet
- Accident Question A IreDocument2 pagesAccident Question A IreMatthew Harris RenfrewNo ratings yet
- UVMC-Amendment Request FormDocument1 pageUVMC-Amendment Request FormMuhammad RosliNo ratings yet
- Parent/Guardian Information: Continued On ReverseDocument2 pagesParent/Guardian Information: Continued On Reverseadhi eng lrtNo ratings yet
- Internal Medicine Consult/New PetsDocument2 pagesInternal Medicine Consult/New PetssequoiavetNo ratings yet
- Around The Clock Childcare LTD Enrollment Form-12rieDocument4 pagesAround The Clock Childcare LTD Enrollment Form-12rieapi-251659956No ratings yet
- Buyer's Information Sheet1Document1 pageBuyer's Information Sheet1VanderBuild Re HoldingsNo ratings yet
- Little Lambs Preschool ApplicationDocument12 pagesLittle Lambs Preschool ApplicationNoopur JainNo ratings yet
- Self Pay Information FormDocument1 pageSelf Pay Information FormPerformax Physical TherapyNo ratings yet
- Fillable Formulario Jovenes Personal and Medical Information SheetDocument2 pagesFillable Formulario Jovenes Personal and Medical Information Sheetrpimerced06No ratings yet
- Detailed Emergency Contact FormDocument2 pagesDetailed Emergency Contact Formandymcgann.mdNo ratings yet
- Ashni: Confidential Information QuestionnaireDocument1 pageAshni: Confidential Information QuestionnairemarinkovikjNo ratings yet
- Post Partum ReportDocument1 pagePost Partum ReportHerald Clarence Martinez AmbayecNo ratings yet
- Teach Children About Stewardship: OctoberDocument4 pagesTeach Children About Stewardship: OctoberStaci InskeepNo ratings yet
- Permission and Release FormDocument1 pagePermission and Release FormStaci InskeepNo ratings yet
- Help Children Build Trust in God: Parenting InsightsDocument4 pagesHelp Children Build Trust in God: Parenting InsightsStaci InskeepNo ratings yet
- Instill A Deep Love For God's Word: AprilDocument4 pagesInstill A Deep Love For God's Word: AprilStaci InskeepNo ratings yet
- Rely On God During Uncertainties: Parenting InsightsDocument4 pagesRely On God During Uncertainties: Parenting InsightsStaci InskeepNo ratings yet
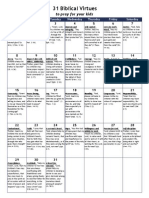
- 31 Biblical Virtues To Pray For Your Children - Calendar FormDocument1 page31 Biblical Virtues To Pray For Your Children - Calendar FormStaci Inskeep100% (1)
- Nurture Your Children's Gifts: MarchDocument4 pagesNurture Your Children's Gifts: MarchStaci InskeepNo ratings yet
- Ways To Watch Your Words: OctoberDocument4 pagesWays To Watch Your Words: OctoberStaci InskeepNo ratings yet
- Loosen The Grip of Materialism: DecemberDocument4 pagesLoosen The Grip of Materialism: DecemberStaci InskeepNo ratings yet
- Help Children Be Grateful Pray-Ers: NovemberDocument4 pagesHelp Children Be Grateful Pray-Ers: NovemberStaci InskeepNo ratings yet
- Teach Children To Love All People: FebruaryDocument4 pagesTeach Children To Love All People: FebruaryStaci InskeepNo ratings yet
- Cryo EnginesDocument6 pagesCryo EnginesgdoninaNo ratings yet
- L1 L2 Highway and Railroad EngineeringDocument7 pagesL1 L2 Highway and Railroad Engineeringeutikol69No ratings yet
- Hager Pricelist May 2014Document64 pagesHager Pricelist May 2014rajinipre-1No ratings yet
- Amare Yalew: Work Authorization: Green Card HolderDocument3 pagesAmare Yalew: Work Authorization: Green Card HolderrecruiterkkNo ratings yet
- ADS 460 Management Principles and Practices: Topic 1: Introduction To ManagementDocument33 pagesADS 460 Management Principles and Practices: Topic 1: Introduction To ManagementNURATIKAH BINTI ZAINOL100% (1)
- Bajaj Allianz InsuranceDocument93 pagesBajaj Allianz InsuranceswatiNo ratings yet
- QA/QC Checklist - Installation of MDB Panel BoardsDocument6 pagesQA/QC Checklist - Installation of MDB Panel Boardsehtesham100% (1)
- 500 Logo Design Inspirations Download #1 (E-Book)Document52 pages500 Logo Design Inspirations Download #1 (E-Book)Detak Studio DesainNo ratings yet
- CoDocument80 pagesCogdayanand4uNo ratings yet
- BASUG School Fees For Indigene1Document3 pagesBASUG School Fees For Indigene1Ibrahim Aliyu GumelNo ratings yet
- PeopleSoft Application Engine Program PDFDocument17 pagesPeopleSoft Application Engine Program PDFSaurabh MehtaNo ratings yet
- Loading N Unloading of Tanker PDFDocument36 pagesLoading N Unloading of Tanker PDFKirtishbose ChowdhuryNo ratings yet
- Job Description For QAQC EngineerDocument2 pagesJob Description For QAQC EngineerSafriza ZaidiNo ratings yet
- Innovations in Land AdministrationDocument66 pagesInnovations in Land AdministrationSanjawe KbNo ratings yet
- QUIZ Group 1 Answer KeyDocument3 pagesQUIZ Group 1 Answer KeyJames MercadoNo ratings yet
- Urun Katalogu 4Document112 pagesUrun Katalogu 4Jose Luis AcevedoNo ratings yet
- Privacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryDocument50 pagesPrivacy: Based On Slides Prepared by Cyndi Chie, Sarah Frye and Sharon Gray. Fifth Edition Updated by Timothy HenryAbid KhanNo ratings yet
- RevisionHistory APFIFF33 To V219Document12 pagesRevisionHistory APFIFF33 To V219younesNo ratings yet
- BluetoothDocument28 pagesBluetoothMilind GoratelaNo ratings yet
- RENCANA KERJA Serious Inspeksi#3 Maret-April 2019Document2 pagesRENCANA KERJA Serious Inspeksi#3 Maret-April 2019Nur Ali SaidNo ratings yet
- Professional Regula/on Commission: Clarita C. Maaño, M.DDocument31 pagesProfessional Regula/on Commission: Clarita C. Maaño, M.Dmiguel triggartNo ratings yet
- Form Three Physics Handbook-1Document94 pagesForm Three Physics Handbook-1Kisaka G100% (1)
- General Diesel Engine Diagnostic Guide PDFDocument3 pagesGeneral Diesel Engine Diagnostic Guide PDFan0th3r_0n3No ratings yet
- SM Land Vs BCDADocument68 pagesSM Land Vs BCDAelobeniaNo ratings yet
- MRT Mrte MRTFDocument24 pagesMRT Mrte MRTFJonathan MoraNo ratings yet
- CSEC Jan 2011 Paper 1Document8 pagesCSEC Jan 2011 Paper 1R.D. KhanNo ratings yet
- HRO (TOOLS 6-9) : Tool 6: My Family and My Career ChoicesDocument6 pagesHRO (TOOLS 6-9) : Tool 6: My Family and My Career ChoicesAkosi EtutsNo ratings yet
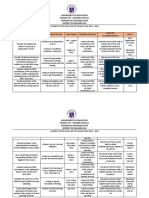
- Action Plan Lis 2021-2022Document3 pagesAction Plan Lis 2021-2022Vervie BingalogNo ratings yet
- Embedded Systems DesignDocument576 pagesEmbedded Systems Designnad_chadi8816100% (4)
- Sky ChemicalsDocument1 pageSky ChemicalsfishNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthFrom EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo ratings yet
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- The Inescapable Immune Escape PandemicFrom EverandThe Inescapable Immune Escape PandemicRating: 5 out of 5 stars5/5 (1)
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (6)
- Sickening: How Big Pharma Broke American Health Care and How We Can Repair ItFrom EverandSickening: How Big Pharma Broke American Health Care and How We Can Repair ItRating: 4 out of 5 stars4/5 (9)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyRating: 4 out of 5 stars4/5 (18)
- Heat Wave: A Social Autopsy of Disaster in ChicagoFrom EverandHeat Wave: A Social Autopsy of Disaster in ChicagoRating: 4 out of 5 stars4/5 (40)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryFrom EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryRating: 4 out of 5 stars4/5 (6)
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthFrom EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthRating: 4 out of 5 stars4/5 (7)
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedNo ratings yet
- Environmental Health and Occupational Health & SafetyFrom EverandEnvironmental Health and Occupational Health & SafetyRating: 3.5 out of 5 stars3.5/5 (9)
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"From EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Rating: 3.5 out of 5 stars3.5/5 (3)
- Breaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeFrom EverandBreaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeNo ratings yet
- The Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceFrom EverandThe Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceNo ratings yet
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (11)
- Healthy Buildings: How Indoor Spaces Drive Performance and ProductivityFrom EverandHealthy Buildings: How Indoor Spaces Drive Performance and ProductivityRating: 5 out of 5 stars5/5 (2)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- Mama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaFrom EverandMama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaNo ratings yet
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadFrom EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadRating: 4.5 out of 5 stars4.5/5 (3)