You might also like
- Global Health in Africa: Historical Perspectives on Disease ControlFrom EverandGlobal Health in Africa: Historical Perspectives on Disease ControlRating: 5 out of 5 stars5/5 (1)
- Community DiagnosisDocument27 pagesCommunity DiagnosisSree Visakh100% (3)
- Epidemiology The Foundation of Public Health PDFDocument34 pagesEpidemiology The Foundation of Public Health PDFgabe18No ratings yet
- NATURAL HISTORY OF DISEASEDocument26 pagesNATURAL HISTORY OF DISEASEadinda mouzasNo ratings yet
- Epidemic Investigation 2Document10 pagesEpidemic Investigation 2Den Anacay100% (1)
- Clinico-Social Case On Tuberculosis: by Shekhar AnandDocument11 pagesClinico-Social Case On Tuberculosis: by Shekhar AnandMike RossNo ratings yet
- Running Head: Pico Question: Aseptic Technique 1Document10 pagesRunning Head: Pico Question: Aseptic Technique 1api-253019091No ratings yet
- EpidemiologyDocument13 pagesEpidemiologyswethashaki50% (2)
- CDC Case Studies in Applied EpidemiologyDocument12 pagesCDC Case Studies in Applied Epidemiologysjab3No ratings yet
- 15-17 - 7-PDF - Community Medicine With Recent Advances - 3 PDFDocument3 pages15-17 - 7-PDF - Community Medicine With Recent Advances - 3 PDFdwimahesaputraNo ratings yet
- Knowledge Attitude and Practice of Mothers Regarding Weaning in Rular Community LahoreDocument6 pagesKnowledge Attitude and Practice of Mothers Regarding Weaning in Rular Community LahorePriyanjali SainiNo ratings yet
- Final exam - infectious disease epidemiologyDocument7 pagesFinal exam - infectious disease epidemiologyIsha Bhatt100% (1)
- The Bamako InitiativeDocument4 pagesThe Bamako Initiativejohn mwangiNo ratings yet
- Maternal Health ServicesDocument24 pagesMaternal Health ServicesMuna Hassan MustafaNo ratings yet
- Community Medicine PDFDocument24 pagesCommunity Medicine PDFEkambaramNo ratings yet
- Health Belief ModelDocument3 pagesHealth Belief ModelWaaberrinNo ratings yet
- Introduction To Reproductive Health, Medical StudentsDocument25 pagesIntroduction To Reproductive Health, Medical StudentsEli Zza KoiralaNo ratings yet
- Community Diagnosis - Ms. Dorothy - 13476Document91 pagesCommunity Diagnosis - Ms. Dorothy - 13476Janet MbandiNo ratings yet
- Hang OutDocument92 pagesHang OutMadhu UpadhyayNo ratings yet
- RN BSN-CIG-Topic 14 - Concepts of Primary Health CareDocument34 pagesRN BSN-CIG-Topic 14 - Concepts of Primary Health CarebettinabetsonNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Approaches To Community Health AssessmentDocument37 pagesApproaches To Community Health AssessmentBetsy Mia Le100% (1)
- Chapter 5: Studying Disease DistributionDocument7 pagesChapter 5: Studying Disease DistributionJohn Rick OrineNo ratings yet
- Urinary Tract Infection Diagnosis and Management For NursesDocument8 pagesUrinary Tract Infection Diagnosis and Management For NursesRonaica InocNo ratings yet
- Natural History of DiseaseDocument11 pagesNatural History of DiseaseAbamvc Muhammad AkbarNo ratings yet
- Basic Measures of EpidemiologyDocument51 pagesBasic Measures of EpidemiologyHafiz SabghatullahNo ratings yet
- Kod Kursus-JIB 533 Nama Kursus: Public Health Nama Pengurus Kursus Dr. Rohayu HamiDocument55 pagesKod Kursus-JIB 533 Nama Kursus: Public Health Nama Pengurus Kursus Dr. Rohayu HamiNurfaizuraNo ratings yet
- Concept of DiseaseDocument80 pagesConcept of DiseaseMamata ManandharNo ratings yet
- OSCE - Breaking Bad NewsDocument2 pagesOSCE - Breaking Bad NewsEman ElzeftawyNo ratings yet
- Sources of Epidemiological Data BoazDocument4 pagesSources of Epidemiological Data Boazgeorgeloto1288% (8)
- Comunity MedicineDocument78 pagesComunity Medicineapi-3831375100% (1)
- Foundations of Nursing PracticeDocument10 pagesFoundations of Nursing PracticeRomeo Casiano Jr.No ratings yet
- Well-Built Clinical Question (PICO)Document32 pagesWell-Built Clinical Question (PICO)noniNo ratings yet
- Mers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDocument25 pagesMers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDaciel GleeNo ratings yet
- Assessment of Attitude of Nursing Mothers Towards Childhood Immunization in Some Selected Communities in Bali, LGA of Taraba StateDocument56 pagesAssessment of Attitude of Nursing Mothers Towards Childhood Immunization in Some Selected Communities in Bali, LGA of Taraba StateJoshua Bature SamboNo ratings yet
- Outbreak InvestigationDocument55 pagesOutbreak InvestigationSumit KarnNo ratings yet
- Chance, Bias, ConfoundingDocument33 pagesChance, Bias, ConfoundingseoukieNo ratings yet
- Community DiagnosisDocument44 pagesCommunity DiagnosisMenuka Shrestha100% (3)
- Family Interventions To Improve Diabetes Outcomes For Adults PDFDocument24 pagesFamily Interventions To Improve Diabetes Outcomes For Adults PDFAfnizar WAhyu RamadhanNo ratings yet
- Epidemiology in Community HealthDocument10 pagesEpidemiology in Community HealthAri Pebrianto AliskaNo ratings yet
- Community Medicine MnemonicsDocument27 pagesCommunity Medicine MnemonicsIzaz KhanNo ratings yet
- Lecture 3 Epidemiology of Intestinal InfectionsDocument46 pagesLecture 3 Epidemiology of Intestinal InfectionsAli Baker AlgelaneNo ratings yet
- 2 Epidemiology TerminologyDocument33 pages2 Epidemiology Terminologynithin shenoiNo ratings yet
- Descriptive Epidemiology Study Types and MethodsDocument34 pagesDescriptive Epidemiology Study Types and Methodslemon yellowNo ratings yet
- Family Health Nursing Process (Final)Document89 pagesFamily Health Nursing Process (Final)Arella FloresNo ratings yet
- Research ProposalDocument21 pagesResearch Proposalapi-351044176No ratings yet
- CHN (1) Community Health NursingDocument1 pageCHN (1) Community Health NursingImation DataNo ratings yet
- GCU 427 Teaching PlanDocument4 pagesGCU 427 Teaching PlanSammy Levuong100% (1)
- RCH program goals for reproductive health and child survivalDocument2 pagesRCH program goals for reproductive health and child survivalAnnapurna DangetiNo ratings yet
- Demography and Family Planning: Community Health Nursing Unit IIDocument49 pagesDemography and Family Planning: Community Health Nursing Unit IIramita sahNo ratings yet
- NCM 112: Care of Client With Inflammatory and Immunologic ResponseDocument10 pagesNCM 112: Care of Client With Inflammatory and Immunologic ResponseNikitaCaitlynLeyaleyNo ratings yet
- Oral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNDocument74 pagesOral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNafrozlakhaniNo ratings yet
- Epidemiology Matching Terms and ActivitiesDocument4 pagesEpidemiology Matching Terms and Activitiesazkha_knowles3279No ratings yet
- Community Diagnosis Sample PDFDocument2 pagesCommunity Diagnosis Sample PDFLisaNo ratings yet
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutFrom EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutRating: 5 out of 5 stars5/5 (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Chronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesFrom EverandChronic Non-communicable Diseases in Ghana: Multidisciplinary PerspectivesNo ratings yet
- Re CSDocument13 pagesRe CSkazulamaNo ratings yet
- Communicable Diseases 2012 Student VersionDocument60 pagesCommunicable Diseases 2012 Student VersionJelaine CENo ratings yet
- B MJ AppendicitisDocument6 pagesB MJ AppendicitisXavier QuinteroNo ratings yet
- Re CSDocument13 pagesRe CSkazulamaNo ratings yet
- Makerere University College of HealthsciencesDocument43 pagesMakerere University College of HealthscienceskazulamaNo ratings yet
- USMLE - BRS Pathology - Flash CardsDocument37 pagesUSMLE - BRS Pathology - Flash CardsJake ChuengNo ratings yet
- NBI Clearance Claim Authorization LetterDocument1 pageNBI Clearance Claim Authorization LetterFrancis Maluntag89% (9)
- NBI Clearance Claim Authorization LetterDocument1 pageNBI Clearance Claim Authorization LetterFrancis Maluntag89% (9)
- Community Diagnosis of The UnicoiDocument11 pagesCommunity Diagnosis of The UnicoikazulamaNo ratings yet
- Pamela Allweiss PPT HRSADocument50 pagesPamela Allweiss PPT HRSAkazulamaNo ratings yet
- CaesareansectionDocument32 pagesCaesareansectionkazulamaNo ratings yet
- What Is Hepatitis ?Document30 pagesWhat Is Hepatitis ?kazulamaNo ratings yet
- Cell Structure & Function GuideDocument26 pagesCell Structure & Function Guideveeramani0% (1)
- HRMDocument19 pagesHRMkazulamaNo ratings yet
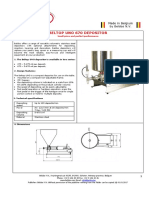
- The Beltop UNO Depositor Is Available in Two SeriesDocument5 pagesThe Beltop UNO Depositor Is Available in Two SeriesJonathan FajardoNo ratings yet
- Formulation of Conditioner-5Document2 pagesFormulation of Conditioner-5TotonMuhammadHenaltonNo ratings yet
- Bio320 Lab 2Document4 pagesBio320 Lab 2Mirza KarmilaNo ratings yet
- Grammar ModuleDocument124 pagesGrammar ModuleMeera Rania100% (1)
- Map of Iowa Club Calf ProducersDocument3 pagesMap of Iowa Club Calf ProducersChristopher AllenNo ratings yet
- Try This! Look Around You.: Directions: Cut Out 10 Food Labels With Nutrition FactsDocument14 pagesTry This! Look Around You.: Directions: Cut Out 10 Food Labels With Nutrition FactsChristine Joy MolinaNo ratings yet
- Jeddah Restaurant MenuDocument8 pagesJeddah Restaurant Menuusama zedanNo ratings yet
- Summary of Current Affais (Dec14-July 15)Document129 pagesSummary of Current Affais (Dec14-July 15)Hari PrakashNo ratings yet
- The Red Data Book On Indian AnimalsDocument555 pagesThe Red Data Book On Indian AnimalspratNo ratings yet
- 14 Couvertures PDFDocument23 pages14 Couvertures PDFAna OrriolsNo ratings yet
- Feasibility Study For PrintDocument39 pagesFeasibility Study For PrintGian Paula Monghit50% (2)
- Giáo Trình Writing Level 4-Đã Chuyển ĐổiDocument80 pagesGiáo Trình Writing Level 4-Đã Chuyển Đổithành trầnNo ratings yet
- Vaidyagrama Ayurveda - Presentation For AsaiDocument25 pagesVaidyagrama Ayurveda - Presentation For AsaiHemalatha PNo ratings yet
- (ThichTiengAnh - Com) de Theo Cau Truc Moi Nam 2017 de 1 Khong Dap AnDocument101 pages(ThichTiengAnh - Com) de Theo Cau Truc Moi Nam 2017 de 1 Khong Dap AnRoland VietnamNo ratings yet
- Knowledge, Attitude and Use of Food Labels Among ConsumersDocument95 pagesKnowledge, Attitude and Use of Food Labels Among ConsumersGodwin KayodeNo ratings yet
- 2018 - Prova - 8 º Ano - 2 º Bimestre - AlineDocument3 pages2018 - Prova - 8 º Ano - 2 º Bimestre - AlineWesley Alves RodriguesNo ratings yet
- FINAL Haggadah 4.1.20Document94 pagesFINAL Haggadah 4.1.20javier romero gonzalezNo ratings yet
- Analytical Methods To Measure The Constants of Fats and Oils-1Document6 pagesAnalytical Methods To Measure The Constants of Fats and Oils-1Zuriel AzametiNo ratings yet
- Plantbased Protein Powder VitacostiqjqkDocument4 pagesPlantbased Protein Powder Vitacostiqjqkprisontaurus7No ratings yet
- Material Sports in The Twenty First Century PDFDocument42 pagesMaterial Sports in The Twenty First Century PDFRubén Darío Gutiérrez PiedrahítaNo ratings yet
- Eat God 0.3Document81 pagesEat God 0.33dgy t33nNo ratings yet
- Krishna's Friend SudamaDocument2 pagesKrishna's Friend SudamaHarshad Ashodiya Interior DesignerNo ratings yet
- PDS08Document675 pagesPDS08fsaharNo ratings yet
- AnalogyDocument73 pagesAnalogyAsh ManakNo ratings yet
- Đề chuẩn minh họa 06 kỳ thi tốt nghiệp THPT năm 2021Document20 pagesĐề chuẩn minh họa 06 kỳ thi tốt nghiệp THPT năm 2021Đăng GiápNo ratings yet
- Separate Mixtures Using Different TechniquesDocument188 pagesSeparate Mixtures Using Different Techniquespankaj16fbNo ratings yet
- Edited Checklist For Fecal EliminationDocument14 pagesEdited Checklist For Fecal EliminationElizalde HusbandNo ratings yet
- Case Study ReportDocument15 pagesCase Study ReportMira SyahirahNo ratings yet
- Can Cant WorksheetDocument2 pagesCan Cant Worksheetjosesita21No ratings yet
- Pengaruh Penambahan Tepung Kunyit Dalam Ransum TerDocument6 pagesPengaruh Penambahan Tepung Kunyit Dalam Ransum TerZulfi Nur Amrina RosyadaNo ratings yet