You might also like
- How to Guide the Apprentice: Temple Garden Tattoo: the Professional StandardFrom EverandHow to Guide the Apprentice: Temple Garden Tattoo: the Professional StandardNo ratings yet
- Great Book of Tattoo Designs, Revised Edition: More than 500 Body Art DesignsFrom EverandGreat Book of Tattoo Designs, Revised Edition: More than 500 Body Art DesignsRating: 4 out of 5 stars4/5 (5)
- Tattoo MachinesDocument11 pagesTattoo MachinesMikistli YowaltekutliNo ratings yet
- Tattoo BookDocument76 pagesTattoo Bookvinh90% (10)
- Polynesian Tattoo Designs: Protection: TattooTribes Design Books, #0From EverandPolynesian Tattoo Designs: Protection: TattooTribes Design Books, #0Rating: 5 out of 5 stars5/5 (2)
- Tattoo Assignment BalanceDocument7 pagesTattoo Assignment Balanceclara8940No ratings yet
- The Mammoth Book of Tattoo PDFDocument560 pagesThe Mammoth Book of Tattoo PDFScott Glacken100% (6)
- Tattoo Aftercare PDFDocument23 pagesTattoo Aftercare PDFtattooaftercare100% (1)
- Tattoo Machine TroubleshootingDocument2 pagesTattoo Machine TroubleshootingMirjana Lukic100% (1)
- Tattooing SafelyDocument16 pagesTattooing Safelyloserboi777No ratings yet
- Tattoo Shading TechniquesDocument5 pagesTattoo Shading Techniquessoyloqueparezco100% (5)
- Complete Tattoo BibleDocument50 pagesComplete Tattoo BibleHelen MushyNo ratings yet
- Tattoo School Training Academy History of TattooingDocument14 pagesTattoo School Training Academy History of TattooingÇağatay SarıkayaNo ratings yet
- Amazing Tattoos For DummiesDocument21 pagesAmazing Tattoos For DummiesMartin Guerra50% (4)
- Kat Von D PrevDocument24 pagesKat Von D PrevƵero Tepes FaithNo ratings yet
- The Complete How To Tattoo GuideDocument18 pagesThe Complete How To Tattoo GuideInkSlave72% (18)
- US768413 Tattoo GunDocument4 pagesUS768413 Tattoo GunEl GrandeNo ratings yet
- Stick and Poke TattooDocument6 pagesStick and Poke TattooRenuka Patra0% (1)
- TattooDocument24 pagesTattooElianeOliveira0% (1)
- Adult Tattoo Consent FormDocument2 pagesAdult Tattoo Consent FormRyan ShmeraNo ratings yet
- 7 Essential Tattoo Tips For Better TattooingDocument15 pages7 Essential Tattoo Tips For Better TattooingMegical Mehandi100% (1)
- Ultimate Tattoo Guide v2Document10 pagesUltimate Tattoo Guide v2Spyros Katsiamakas100% (2)
- Tattoo WorsheetDocument1 pageTattoo Worsheetapi-298984519No ratings yet
- Tattoo Machine ManualDocument20 pagesTattoo Machine ManualDimas Candido Ferreira100% (1)
- Tattoo After CareDocument1 pageTattoo After CareLane von CassidyNo ratings yet
- Pen & Ink: Tattoos and the Stories Behind ThemFrom EverandPen & Ink: Tattoos and the Stories Behind ThemRating: 4 out of 5 stars4/5 (25)
- Training Manual For The Tattoo ArtistDocument67 pagesTraining Manual For The Tattoo ArtistMartin Coyle100% (2)
- Total Tattoo-June 2021Document114 pagesTotal Tattoo-June 2021Comicgek100% (2)
- TattooDocument124 pagesTattooHielkePost100% (7)
- Tattoo: Book of SecretsDocument15 pagesTattoo: Book of SecretsSteveSalvatori80% (5)
- Tattoo WSDocument22 pagesTattoo WSAnonymous 9glfmx3No ratings yet
- Tattoo Encyclopedia: A Guide to Choosing Your TattooFrom EverandTattoo Encyclopedia: A Guide to Choosing Your TattooRating: 3.5 out of 5 stars3.5/5 (23)
- GET The Perfect TattooDocument11 pagesGET The Perfect TattoomarzstarNo ratings yet
- Tattoo VectorsDocument9 pagesTattoo VectorsdenizzleNo ratings yet
- Solong Catalogue-2022Document113 pagesSolong Catalogue-2022David AnthonyNo ratings yet
- Customizing the Body: The Art and Culture of TattooingFrom EverandCustomizing the Body: The Art and Culture of TattooingRating: 4 out of 5 stars4/5 (5)
- Shadowing Journals Tattooing and PiercingsDocument6 pagesShadowing Journals Tattooing and Piercingsapi-490186008No ratings yet
- Tattoo - WikipediaDocument18 pagesTattoo - WikipediaJaime AdrianNo ratings yet
- Tattoo BBBDocument27 pagesTattoo BBBFran SilvaNo ratings yet
- A Complete Tattoo Studio Business Plan: A Key Part Of How To Start A Tattoo Parlor & Body Piercing BusinessFrom EverandA Complete Tattoo Studio Business Plan: A Key Part Of How To Start A Tattoo Parlor & Body Piercing BusinessNo ratings yet
- Tattoo Studios RegulationDocument15 pagesTattoo Studios RegulationPanama Inked AkiNo ratings yet
- Artist's Collections - Kingpin Tattoo Supply (PDFDrive) PDFDocument92 pagesArtist's Collections - Kingpin Tattoo Supply (PDFDrive) PDFSalim Helo0% (1)
- Romaninan Tattoo News No 4Document34 pagesRomaninan Tattoo News No 4Reviste onlineNo ratings yet
- How To Get The Perfect Tattoo PDFDocument11 pagesHow To Get The Perfect Tattoo PDFSebastian GuevaraNo ratings yet
- Tattoo Consent Form MinorDocument1 pageTattoo Consent Form MinorafkjdkfjslkfjdklNo ratings yet
- Gamborg PDFDocument72 pagesGamborg PDFAlexandra CastroNo ratings yet
- Nebraska Public Service Commission's Decision On Keystone XLDocument74 pagesNebraska Public Service Commission's Decision On Keystone XLcaleyramsayNo ratings yet
- Opioids Substances Misuse Report 2017 Q3Document27 pagesOpioids Substances Misuse Report 2017 Q3caleyramsayNo ratings yet
- Alberta Health Services Inspection Report of Lethbridge Burger KingDocument3 pagesAlberta Health Services Inspection Report of Lethbridge Burger KingcaleyramsayNo ratings yet
- Opioids Substances Misuse Report 2017 Q1 FinalDocument24 pagesOpioids Substances Misuse Report 2017 Q1 FinalcaleyramsayNo ratings yet
- Marijuana GuidelinesDocument10 pagesMarijuana GuidelinesCanoe.comNo ratings yet
- Growth Monitoring Report 2017Document96 pagesGrowth Monitoring Report 2017caleyramsayNo ratings yet
- Stone Versus Crouse RulingDocument16 pagesStone Versus Crouse RulingcaleyramsayNo ratings yet
- Conference Board of Canada ReportDocument230 pagesConference Board of Canada ReportcaleyramsayNo ratings yet
- Edmonton's Updated Plan To Prevent and End HomelessnessDocument82 pagesEdmonton's Updated Plan To Prevent and End HomelessnesscaleyramsayNo ratings yet
- Alberta Foster Boy Kawliga Potts Fatality ReportDocument20 pagesAlberta Foster Boy Kawliga Potts Fatality ReportcaleyramsayNo ratings yet
- Traffic Transport Parking EssentialsDocument17 pagesTraffic Transport Parking EssentialscaleyramsayNo ratings yet
- The Parliamentary Budget Office's Fiscal Sustainability Report 2017Document125 pagesThe Parliamentary Budget Office's Fiscal Sustainability Report 2017caleyramsayNo ratings yet
- WCB Review Final ReportDocument192 pagesWCB Review Final ReportcaleyramsayNo ratings yet
- Century Park Park and Ride ChangesDocument1 pageCentury Park Park and Ride ChangescaleyramsayNo ratings yet
- Cyclist and Pedestrian Safety Action Plan - June 12 2017Document6 pagesCyclist and Pedestrian Safety Action Plan - June 12 2017caleyramsayNo ratings yet
- Ty's Exotics Press ReleaseDocument5 pagesTy's Exotics Press ReleasecaleyramsayNo ratings yet
- Letter Sent To Ryley Residents Tuesday, Feb. 21, 2017Document3 pagesLetter Sent To Ryley Residents Tuesday, Feb. 21, 2017caleyramsayNo ratings yet
- Alberta Economic Outlook May 2017Document10 pagesAlberta Economic Outlook May 2017caleyramsayNo ratings yet
- Opioids Substances Misuse Report 2017 Q1 FinalDocument24 pagesOpioids Substances Misuse Report 2017 Q1 FinalcaleyramsayNo ratings yet
- Legal Documents Filed by Alberta EnvironmentDocument2 pagesLegal Documents Filed by Alberta EnvironmentcaleyramsayNo ratings yet
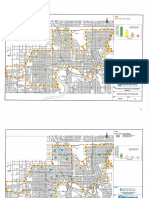
- City of Edmonton Flood MapsDocument32 pagesCity of Edmonton Flood MapsedmontonjournalNo ratings yet
- 2016 Edmonton Vital Signs ReportDocument8 pages2016 Edmonton Vital Signs ReportcaleyramsayNo ratings yet
- Wildfire MNP ReportDocument92 pagesWildfire MNP Reportcaleyramsay100% (2)
- Used Car Seat Check ListDocument1 pageUsed Car Seat Check ListcaleyramsayNo ratings yet
- Boil Water AdvisoryDocument1 pageBoil Water AdvisorycaleyramsayNo ratings yet
- Lifesaving Society's 2016 Alberta Drowning ReportDocument4 pagesLifesaving Society's 2016 Alberta Drowning ReportcaleyramsayNo ratings yet
- Fort McMurray Wildfire: Re-Entry Timeline and MapDocument1 pageFort McMurray Wildfire: Re-Entry Timeline and MapcaleyramsayNo ratings yet
- Low Income Transit Pass EdmontonDocument2 pagesLow Income Transit Pass EdmontoncaleyramsayNo ratings yet
- Low Income Transit Pass EdmontonDocument2 pagesLow Income Transit Pass EdmontoncaleyramsayNo ratings yet
- BandagingDocument12 pagesBandagingJUANJOSEFOXNo ratings yet
- University of The Philippines College of Law: RD RDDocument2 pagesUniversity of The Philippines College of Law: RD RDMaribel Nicole LopezNo ratings yet
- Ergonomics Awareness Education For Employees and SupervisorsDocument71 pagesErgonomics Awareness Education For Employees and SupervisorsramseyNo ratings yet
- Ardhamatsyendra & HalasanDocument13 pagesArdhamatsyendra & HalasangauravNo ratings yet
- Omsite 2004 PDFDocument196 pagesOmsite 2004 PDFJulieNo ratings yet
- BSG - tp01 - SW - 07004 - Rev 00 Swms For Bored PileDocument10 pagesBSG - tp01 - SW - 07004 - Rev 00 Swms For Bored Pilekhairul barsriNo ratings yet
- St. Mary's Academy Case DigestDocument4 pagesSt. Mary's Academy Case DigestMicaela Dela PeñaNo ratings yet
- Q2 Lesson 7Document25 pagesQ2 Lesson 7mint hvryNo ratings yet
- Sepsis Notes Amended On 24th Feb 2019Document31 pagesSepsis Notes Amended On 24th Feb 2019Ereny66No ratings yet
- NCLEX-RN Cheat Sheet (Claudia Goncalves)Document14 pagesNCLEX-RN Cheat Sheet (Claudia Goncalves)Rovie Gonzales Dimas100% (33)
- How To Ensure Safety For Castable MixingDocument4 pagesHow To Ensure Safety For Castable MixingNaelNo ratings yet
- 6 X 48 Belt Disc SanderDocument20 pages6 X 48 Belt Disc SanderJ DavisNo ratings yet
- Only Time Series by XieDocument494 pagesOnly Time Series by XiepharaveejNo ratings yet
- Neuropsychological Studies of The Frontal LobesDocument26 pagesNeuropsychological Studies of The Frontal LobesIcaroNo ratings yet
- Petronas Risk Matrix ProcedureDocument16 pagesPetronas Risk Matrix Procedureme_lokie100% (1)
- Performing Chest PhysiotherapyDocument14 pagesPerforming Chest PhysiotherapyDivya Chauhan100% (1)
- Nnadili v. Chevron U.s.a., Inc.Document10 pagesNnadili v. Chevron U.s.a., Inc.RavenFoxNo ratings yet
- Exercises and ArticlesDocument37 pagesExercises and Articlesgizzy9dillespieNo ratings yet
- Gadar 220190401Document7 pagesGadar 220190401muhammad pratamaNo ratings yet
- HomeopathyDocument16 pagesHomeopathygregotza0% (1)
- Simpson Performance Products v. D.J. SafetyDocument6 pagesSimpson Performance Products v. D.J. SafetyPriorSmartNo ratings yet
- Triage QuizDocument11 pagesTriage QuizJoshua Flores Fernan100% (1)
- CCB Indian Railways Locomotive Maintenance ManualDocument4 pagesCCB Indian Railways Locomotive Maintenance ManualumadeviNo ratings yet
- Legal and TaxDocument35 pagesLegal and TaxSachin MethreeNo ratings yet
- Airbags and Collisions EssayDocument2 pagesAirbags and Collisions EssayDianaNo ratings yet
- Frog AtlasDocument26 pagesFrog AtlasAlelie Ayen100% (2)
- Art of Fitness BrochureDocument62 pagesArt of Fitness Brochureprotein47No ratings yet
- Kulkarni2012 PDFDocument7 pagesKulkarni2012 PDFAby SuryaNo ratings yet
- Health and Safety Manual FINALDocument61 pagesHealth and Safety Manual FINALbmarsh10100% (2)
- Backseat Inclination Affects The Myoelectric.252Document5 pagesBackseat Inclination Affects The Myoelectric.252Lina M GarciaNo ratings yet