You might also like
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionFrom EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionNo ratings yet
- Occupation Based InterventionsDocument16 pagesOccupation Based Interventionsapi-293182319100% (1)
- PDT PlanDocument2 pagesPDT Planapi-283869583No ratings yet
- Allen Cognitive Level ScreenDocument9 pagesAllen Cognitive Level ScreenIntan Indah Sari100% (2)
- Quick DASHDocument4 pagesQuick DASHKennedy Hindley100% (1)
- Ampsmanual Chapters1-4Document52 pagesAmpsmanual Chapters1-4Aymen DabboussiNo ratings yet
- Working As An Occupational Therapist in Another Country 2015Document101 pagesWorking As An Occupational Therapist in Another Country 2015RLedgerdNo ratings yet
- Frame of ReferenceDocument10 pagesFrame of ReferenceGustavo CabanasNo ratings yet
- Initial TemplateDocument8 pagesInitial TemplateZuj PayNo ratings yet
- OT Self Care Modified Barthel IndexDocument4 pagesOT Self Care Modified Barthel Indexlolocy LNo ratings yet
- Instrumental Activities Daily Living: Try ThisDocument11 pagesInstrumental Activities Daily Living: Try ThisbalryoNo ratings yet
- Artifact 5 Soap NoteDocument3 pagesArtifact 5 Soap Noteapi-517998988No ratings yet
- PT GoalsDocument13 pagesPT Goalsnaomi harowNo ratings yet
- Presented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDocument22 pagesPresented By: Ashlee Barbeau Student Occupational Therapist, Queen's UniversityDanielle Stella N'LucaNo ratings yet
- Occupational Therapy and Mental Health 1Document18 pagesOccupational Therapy and Mental Health 1Roman -No ratings yet
- Functional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUDocument15 pagesFunctional Assessment: DR Sonali Soumyashree BPT, MPT (Neurology) Lecturer, GDGUSonali Soumyashree100% (2)
- Rehabilitative Frame of Reference-1Document18 pagesRehabilitative Frame of Reference-1Caryssa Vitelli100% (1)
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Document54 pages2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18No ratings yet
- Soap 11Document4 pagesSoap 11api-436429414No ratings yet
- StrokeDocument5 pagesStrokeapi-261670650No ratings yet
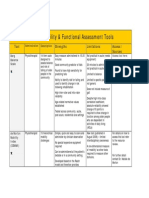
- Mobility and Functional Assessment ToolsDocument4 pagesMobility and Functional Assessment Toolssonya63265No ratings yet
- Aota PDFDocument2 pagesAota PDFJuliana MassariolliNo ratings yet
- Work and Occupational TherapyDocument31 pagesWork and Occupational Therapysmith197077No ratings yet
- Position Paper OT For People With LDDocument10 pagesPosition Paper OT For People With LDLytiana WilliamsNo ratings yet
- OT Practice December 17 IssueDocument24 pagesOT Practice December 17 IssueThe American Occupational Therapy Association100% (1)
- Soap NoteDocument2 pagesSoap Noteapi-285542134No ratings yet
- The Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeDocument55 pagesThe Application of Assessment and Evaluation Procedure in Using Occupation Centered PracticeAswathi100% (2)
- Wrist Hand OrthosisDocument3 pagesWrist Hand OrthosisKhageswar SamalNo ratings yet
- 10 - Mood & Anxiety MeasuresDocument36 pages10 - Mood & Anxiety MeasuresopiknrNo ratings yet
- Otor & Visual Motor AssessDocument4 pagesOtor & Visual Motor AssessBea FloresNo ratings yet
- A.5 Assessment PowerPoint 2016Document38 pagesA.5 Assessment PowerPoint 2016Ptrc Lbr LpNo ratings yet
- App1 Pain Rating ScalesDocument4 pagesApp1 Pain Rating Scalesthilaga88No ratings yet
- The Canadian Model of Occupational Performance and EngagementDocument16 pagesThe Canadian Model of Occupational Performance and Engagementalepati29No ratings yet
- Clients Goals To Address in SessionDocument8 pagesClients Goals To Address in Sessionapi-436429414No ratings yet
- H Clinical Assessment ToolsDocument71 pagesH Clinical Assessment ToolsPaijo SusenoNo ratings yet
- Strategies Used by Occupational Therapy To Maximize ADL IndependenceDocument53 pagesStrategies Used by Occupational Therapy To Maximize ADL IndependenceNizam lotfiNo ratings yet
- Dickson Occupational ProfileDocument18 pagesDickson Occupational Profileapi-255001706No ratings yet
- Occupational AdaptationDocument5 pagesOccupational AdaptationVASH12345100% (1)
- Soap NoteDocument1 pageSoap Noteapi-519577267No ratings yet
- Allen Cognitive Level Testreport 1Document27 pagesAllen Cognitive Level Testreport 1Kimmy ChuNo ratings yet
- Barthel IndexDocument4 pagesBarthel IndexrlinaoNo ratings yet
- The Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityDocument7 pagesThe Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityIJAR JOURNALNo ratings yet
- Pediatric Comm Client SoapDocument4 pagesPediatric Comm Client Soapapi-580425291No ratings yet
- Dementia AOTA Helpful Fact SheetDocument2 pagesDementia AOTA Helpful Fact SheetMysti Reeder100% (1)
- OT Models PratciceDocument30 pagesOT Models PratciceWalaa Eldesoukey100% (1)
- Occupational Therapy As A Major Activity of Human Being: by Rafia KhalidDocument20 pagesOccupational Therapy As A Major Activity of Human Being: by Rafia Khalidnomi9818No ratings yet
- Ota Group ProtocolDocument26 pagesOta Group Protocolapi-318685839No ratings yet
- Sensory Processing Disorders - Diagnostic and Therapeutic ControversiesDocument10 pagesSensory Processing Disorders - Diagnostic and Therapeutic ControversiesiimNo ratings yet
- Occt630 Occupational Profile InterventionDocument19 pagesOcct630 Occupational Profile Interventionapi-290880850No ratings yet
- SP2 Short Form and Caregiver Template Summary & Interpretation FormDocument4 pagesSP2 Short Form and Caregiver Template Summary & Interpretation FormjcNo ratings yet
- The+Model+of+Creative+AbilityDocument22 pagesThe+Model+of+Creative+AbilitysandeepNo ratings yet
- Ashley M Occt 651 Occupational ProfileDocument11 pagesAshley M Occt 651 Occupational Profileapi-25080062950% (2)
- PTH 870-Occupational TherapyDocument13 pagesPTH 870-Occupational Therapyapi-551496110100% (1)
- Home Environmental AssessmentDocument2 pagesHome Environmental AssessmentSelvi Puspa SariNo ratings yet
- 2012 Practice Analysis Executive Otr PDFDocument32 pages2012 Practice Analysis Executive Otr PDFRuxandra PredaNo ratings yet
- Occt 652a - ResumeDocument3 pagesOcct 652a - Resumeapi-279916752No ratings yet
- Assessment of HandDocument76 pagesAssessment of Handchirag0% (1)
- Contoh Ot ReportDocument10 pagesContoh Ot ReportHanum HamkaNo ratings yet
- Spinal Cord Assesment Form PTDocument8 pagesSpinal Cord Assesment Form PTSureaka PonnusamyNo ratings yet
- CC StrokeDocument13 pagesCC Strokeapi-436090845100% (1)
- Touro University Nevada Occupational Therapy My PerformanceDocument6 pagesTouro University Nevada Occupational Therapy My Performanceapi-239817112No ratings yet
- Group Presentation Occt 655Document60 pagesGroup Presentation Occt 655api-239817112No ratings yet
- Touro University Nevada Occupational Therapy My PerformanceDocument5 pagesTouro University Nevada Occupational Therapy My Performanceapi-239817112No ratings yet
- Resume Mar 4Document2 pagesResume Mar 4api-239817112No ratings yet
- Occt 650 Outline For Lead Dev PlanDocument6 pagesOcct 650 Outline For Lead Dev Planapi-239817112No ratings yet
- Occt 643 Cat Template 1Document10 pagesOcct 643 Cat Template 1api-239817112No ratings yet
- At DeviceDocument12 pagesAt Deviceapi-239817112No ratings yet
- Cat Evidence Table Worksheet FinalDocument10 pagesCat Evidence Table Worksheet Finalapi-239817112No ratings yet
- Thejourneytograduateschool PaperDocument12 pagesThejourneytograduateschool Paperapi-239817112No ratings yet
- Styles of CitationDocument4 pagesStyles of CitationFranz Regie BlancoNo ratings yet
- Creating Learning Environments - PaperDocument1 pageCreating Learning Environments - PaperMinNo ratings yet
- Henry MurrayDocument16 pagesHenry MurrayLouriel NopalNo ratings yet
- Board Examination Sample QuestionsDocument11 pagesBoard Examination Sample QuestionsStranded JavaNo ratings yet
- PreviewpdfDocument58 pagesPreviewpdfprincessNo ratings yet
- Understanding Communication: The Value of CommunicationDocument4 pagesUnderstanding Communication: The Value of CommunicationInterfaith CarePartnersNo ratings yet
- What Is Coach Education.: Individual CoachingDocument7 pagesWhat Is Coach Education.: Individual CoachingOragon Dum Spiro SperoNo ratings yet
- DISSOCIATIVE DISORDERS - TeachersDocument19 pagesDISSOCIATIVE DISORDERS - TeachersIano IanoNo ratings yet
- MGT502 Important 565 MCQ's Collected by Askari Team . 100% Sure SolvedDocument149 pagesMGT502 Important 565 MCQ's Collected by Askari Team . 100% Sure SolvedMalikusmanNo ratings yet
- Humanistic TheoryDocument28 pagesHumanistic TheoryNano KaNo ratings yet
- Self-Learning Module: Grade 7Document6 pagesSelf-Learning Module: Grade 7NicxNo ratings yet
- Spring 2023 - EDU302 - 1 1Document5 pagesSpring 2023 - EDU302 - 1 1zohaNo ratings yet
- Article CritiqueDocument8 pagesArticle Critiqueapi-220585177No ratings yet
- Sexuality in The 21st Century, Sexual Fluidity. Bhugra (2019)Document5 pagesSexuality in The 21st Century, Sexual Fluidity. Bhugra (2019)Aylin Lidsay Feria GNo ratings yet
- Ethical CommunicationDocument3 pagesEthical CommunicationDavis SamNo ratings yet
- Ethical LeadershipDocument17 pagesEthical LeadershipThant AungNo ratings yet
- Final ExaminationsDocument4 pagesFinal ExaminationsRocky RabinoNo ratings yet
- Lecture 3 CognitivismDocument48 pagesLecture 3 Cognitivismbella100% (1)
- Self Leadership AssignmentDocument7 pagesSelf Leadership AssignmentGiles CreelmanNo ratings yet
- Narcissistic Parents and Recommended Reading PDFDocument4 pagesNarcissistic Parents and Recommended Reading PDFAlin Apostolescu50% (2)
- HRM Week 2Document18 pagesHRM Week 2doll3kittenNo ratings yet
- Materi - Method and Approaches in HPDocument98 pagesMateri - Method and Approaches in HPdiniindahlestariNo ratings yet
- A Correlational Study of The Relationship BetweenDocument11 pagesA Correlational Study of The Relationship BetweenAlfath MarzukiNo ratings yet
- The Fairy Tale TestDocument5 pagesThe Fairy Tale TestBóbita BabaklubNo ratings yet
- Grievance ProcedureDocument11 pagesGrievance ProcedureApeksha TiwariNo ratings yet
- Gender SensitivityDocument32 pagesGender SensitivityMiguel Lemuel De Mesa100% (4)
- Research Paper Final Stem 112Document16 pagesResearch Paper Final Stem 112Daniel NevadoNo ratings yet
- Horwitzetal 1986 FLClassroom Anxiety ScaleDocument9 pagesHorwitzetal 1986 FLClassroom Anxiety ScalepmacgregNo ratings yet
- Antje Diedrich - Last in A Long Line of Literary Kleptomaniacs. Intertextuality in Sarah Kane's 4.48 PsychosisDocument26 pagesAntje Diedrich - Last in A Long Line of Literary Kleptomaniacs. Intertextuality in Sarah Kane's 4.48 PsychosisCaro MNo ratings yet
- About Art Therapy and SchoolsDocument4 pagesAbout Art Therapy and SchoolsJay-ar BaybayNo ratings yet
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthFrom EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo ratings yet
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (6)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthFrom EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthRating: 4 out of 5 stars4/5 (7)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (11)
- Summary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public Health by Robert F. Kennedy Jr: Key Takeaways, Summary & Analysis IncludedNo ratings yet
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyRating: 4 out of 5 stars4/5 (18)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- The Inescapable Immune Escape PandemicFrom EverandThe Inescapable Immune Escape PandemicRating: 5 out of 5 stars5/5 (1)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryFrom EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryRating: 4 out of 5 stars4/5 (6)
- The Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceFrom EverandThe Wuhan Cover-Up: And the Terrifying Bioweapons Arms RaceNo ratings yet
- Heat Wave: A Social Autopsy of Disaster in ChicagoFrom EverandHeat Wave: A Social Autopsy of Disaster in ChicagoRating: 4 out of 5 stars4/5 (40)
- Profiles of the Vaccine-Injured: "A Lifetime Price to Pay"From EverandProfiles of the Vaccine-Injured: "A Lifetime Price to Pay"Rating: 3.5 out of 5 stars3.5/5 (3)
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- Vaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadFrom EverandVaccines Did Not Cause Rachel's Autism: My Journey as a Vaccine Scientist, Pediatrician, and Autism DadRating: 4.5 out of 5 stars4.5/5 (3)
- Mama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaFrom EverandMama Might Be Better Off Dead: The Failure of Health Care in Urban AmericaNo ratings yet
- Community-Acquired Pneumonia: Strategies for ManagementFrom EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresRating: 4.5 out of 5 stars4.5/5 (2)
- Breaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeFrom EverandBreaking out of the Health Care Abyss: Transformational Tips for Agents of ChangeNo ratings yet
- Healthy Buildings: How Indoor Spaces Drive Performance and ProductivityFrom EverandHealthy Buildings: How Indoor Spaces Drive Performance and ProductivityRating: 5 out of 5 stars5/5 (2)