You might also like
- Concept 1 - Leadership & Management in NursingDocument652 pagesConcept 1 - Leadership & Management in Nursingezenz0205100% (3)
- NCM 105 Nursing Leadership and ManagementDocument295 pagesNCM 105 Nursing Leadership and ManagementMica Ann Dela Cruz100% (3)
- LEC 1 PRELIM Nursing Leadership and ManagementDocument307 pagesLEC 1 PRELIM Nursing Leadership and ManagementMae Montesena BreganzaNo ratings yet
- Task-Oriented Relationship-Oriented Participative Leadership Task-OrientedDocument17 pagesTask-Oriented Relationship-Oriented Participative Leadership Task-OrientedDENNIS N. MUÑOZNo ratings yet
- Nursing Leadership and ManagementDocument182 pagesNursing Leadership and ManagementAlain Dave90% (10)
- Nursing Leadership & ManagementDocument36 pagesNursing Leadership & ManagementPrince Paraiso100% (7)
- Nursing Leadership and ManagementDocument13 pagesNursing Leadership and ManagementChrisgr8100% (6)
- Nursing Leadership and Management Prelims Lesson 1-5Document4 pagesNursing Leadership and Management Prelims Lesson 1-5Paul Christian P. Santos, RN100% (14)
- Nursing Leadership and ManagementDocument8 pagesNursing Leadership and Managementaurezea50% (2)
- Unit 1 Chapter 2 Nursing Leadership and ManagementDocument9 pagesUnit 1 Chapter 2 Nursing Leadership and Managementfree_books_jym100% (1)
- Nursing Management 2Document118 pagesNursing Management 2Jasmin Jacob100% (36)
- Nursing Leadership and Management PDFDocument10 pagesNursing Leadership and Management PDFhahahahaaaaaaa100% (9)
- Nursing Leadership and ManagementDocument43 pagesNursing Leadership and Managementbajaoc95% (22)
- Leadership and ManagementDocument216 pagesLeadership and ManagementYum C75% (4)
- Nursing Leadership and Management ExamsDocument4 pagesNursing Leadership and Management ExamsMarisol Jane Jomaya67% (9)
- Nursing Leadership and ManagementDocument48 pagesNursing Leadership and ManagementDarl DacdacNo ratings yet
- Nursing Leadership - Reviewquestion 1Document6 pagesNursing Leadership - Reviewquestion 1Darren Jay Nikazy80% (5)
- Nursing Management & LeadershipDocument8 pagesNursing Management & LeadershipDjhoanna Kriska88% (42)
- Nursing ManagementDocument24 pagesNursing ManagementSimran Josan100% (1)
- NURSING Management ProcessDocument80 pagesNURSING Management Processma_tabora628391% (33)
- Nursing Management LeadershipDocument8 pagesNursing Management LeadershipIvy Balza Caber100% (1)
- Nursing Leadership and ManagementDocument3 pagesNursing Leadership and ManagementRI NA100% (1)
- Nursing Leadership TheoriesDocument121 pagesNursing Leadership TheoriesHoneylet Villanueva67% (3)
- Controlling in Nursing ManagementDocument45 pagesControlling in Nursing Managementverna92% (37)
- NLM QuestionsDocument15 pagesNLM Questionsleoboi_leoboi81% (16)
- Nursing Management Process and FunctionsDocument151 pagesNursing Management Process and FunctionsJaq Kyatchon90% (29)
- Leadership and Management in NursingDocument5 pagesLeadership and Management in NursingSolsona Natl HS Maananteng100% (1)
- Nursing Management - Concepts and Principles of ManagementDocument4 pagesNursing Management - Concepts and Principles of Managementsoundaramilangovan254989% (9)
- Directing in Nursing ManagementDocument27 pagesDirecting in Nursing Managementwersken100% (4)
- The Organizational Structure of Nursing Service DepartmentDocument5 pagesThe Organizational Structure of Nursing Service DepartmentNikki Arra100% (8)
- Leadership and ManagementDocument24 pagesLeadership and Managementansh2195100% (2)
- Lec Note - NSG Leadership and ManagementDocument86 pagesLec Note - NSG Leadership and Managementederlyn21No ratings yet
- CBQ - Leadership and Management in Nursing 2009Document14 pagesCBQ - Leadership and Management in Nursing 2009Lizette Leah Ching95% (20)
- Nursing Leadership NCM 105: Madeline N. Gerzon, RN, MM Clinical InstructorDocument74 pagesNursing Leadership NCM 105: Madeline N. Gerzon, RN, MM Clinical Instructormgerzon93% (15)
- Nursing Leadership and Management Practice TestDocument6 pagesNursing Leadership and Management Practice TestHaifi Hun0% (1)
- ControllingDocument8 pagesControllingAnjo Pasiolco Canicosa100% (2)
- Nursing AdministrationDocument71 pagesNursing AdministrationJoYCe100% (5)
- Organizing Management NursingDocument31 pagesOrganizing Management NursingAlfitoHarfahGiffary100% (1)
- Leadership in NursingDocument31 pagesLeadership in NursingMichael Urrutia100% (1)
- Leadership and Managementfinal Nursing ReviewerDocument23 pagesLeadership and Managementfinal Nursing ReviewerPhilip Simangan100% (5)
- DelegationDocument58 pagesDelegationkrishnasree100% (1)
- Nursing Management IntroductionDocument42 pagesNursing Management Introductionanreilegarde100% (5)
- Midterm Leadership and Management (MCN 107) EXAMDocument26 pagesMidterm Leadership and Management (MCN 107) EXAMsophi30100% (1)
- LMR Notes 1Document15 pagesLMR Notes 1Krisly Jade TeoNo ratings yet
- Educational LeadershipDocument46 pagesEducational LeadershipNiño Angelo AustriaNo ratings yet
- Being An Effective LeaderDocument19 pagesBeing An Effective LeaderHamza AliNo ratings yet
- LeadershipDocument53 pagesLeadershipcute_little4596% (72)
- Leadership and ManagementDocument5 pagesLeadership and ManagementYmon TuallaNo ratings yet
- What Is Your Personaldefinition of Leadership? Definition of LeadershipDocument11 pagesWhat Is Your Personaldefinition of Leadership? Definition of LeadershipAnnaMae MalapitNo ratings yet
- Leadershi P: Group 4 - Nazareno, Jhonsin E. - Tudon, Sittie Raiza Bantas - Sali, Alta-Abbon Mamako - Ibrahim, Madani GDocument28 pagesLeadershi P: Group 4 - Nazareno, Jhonsin E. - Tudon, Sittie Raiza Bantas - Sali, Alta-Abbon Mamako - Ibrahim, Madani GHazel Mae JumaaniNo ratings yet
- Hbo Chapter 8 - LeadershipDocument72 pagesHbo Chapter 8 - LeadershipAbegail Perez100% (1)
- LeadingDocument6 pagesLeadingdummyNo ratings yet
- Em 502 LeadershipDocument4 pagesEm 502 LeadershipAngelie CayananNo ratings yet
- Leadership & ManagementDocument83 pagesLeadership & ManagementJasmin Jacob92% (13)
- Leadership & Influence ProcessDocument43 pagesLeadership & Influence ProcessAnnalene de guzmanNo ratings yet
- LeadershipDocument6 pagesLeadershipayubwasongaNo ratings yet
- Hbo Chapter 8 ReportDocument72 pagesHbo Chapter 8 ReportAbegail PerezNo ratings yet
- LeadershipDocument2 pagesLeadershipNeha KanojiyaNo ratings yet
- Leadership: Leadership Is The Ability To Influence A Group Toward The Achievement of A Vision or Set of GoalsDocument5 pagesLeadership: Leadership Is The Ability To Influence A Group Toward The Achievement of A Vision or Set of GoalsSadia RasoolNo ratings yet
- (Front and Back Page) It 23 ProjectDocument2 pages(Front and Back Page) It 23 Projectpaul andrew laranjo asuncionNo ratings yet
- DiabetesDocument2 pagesDiabetespaul andrew laranjo asuncionNo ratings yet
- Mathematics CoverDocument3 pagesMathematics Coverpaul andrew laranjo asuncionNo ratings yet
- PathophysiologyDocument9 pagesPathophysiologypaul andrew laranjo asuncionNo ratings yet
- Front Page.Document1 pageFront Page.paul andrew laranjo asuncionNo ratings yet
- Nursing ManagementDocument38 pagesNursing Managementpaul andrew laranjo asuncion100% (1)
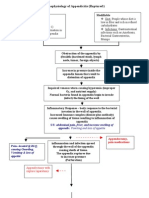
- Pathophysiology of Appendicitis (Ruptured)Document2 pagesPathophysiology of Appendicitis (Ruptured)paul andrew laranjo asuncion100% (2)
- Pathophysiology of Neonatal Sepsis Secondary To Neonatal PneumoniaDocument4 pagesPathophysiology of Neonatal Sepsis Secondary To Neonatal Pneumoniapaul andrew laranjo asuncion80% (5)
- Target User Persona: Primary ConcernsDocument4 pagesTarget User Persona: Primary ConcernsNtinaGanesNo ratings yet
- Book Review FormatDocument3 pagesBook Review Formatmisseuhlicious100% (5)
- S2 2016 372985 Bibliography PDFDocument2 pagesS2 2016 372985 Bibliography PDFNanang AriesNo ratings yet
- Why Battered Women Do Not Leave, Part 2Document33 pagesWhy Battered Women Do Not Leave, Part 2danielaNo ratings yet
- Modicare and Its ImpactDocument9 pagesModicare and Its ImpactsagarNo ratings yet
- Trademark & DesignsDocument22 pagesTrademark & DesignsHimanshu GoelNo ratings yet
- Tancinco V GSISDocument3 pagesTancinco V GSISDenzoNo ratings yet
- Chapter 1 - Eco Adventure ParkDocument16 pagesChapter 1 - Eco Adventure ParkLei RamosNo ratings yet
- Assignment AnswersDocument35 pagesAssignment AnswersShine k100% (1)
- Social Science 4 Byme Unit 5Document3 pagesSocial Science 4 Byme Unit 5Noelia Martínez Colmenar50% (2)
- List The Elements of A New-Venture Team?Document11 pagesList The Elements of A New-Venture Team?Amethyst OnlineNo ratings yet
- Assignment 7Document16 pagesAssignment 7Anik Kumar MallickNo ratings yet
- Early Identification and Screening: Definition of Developmental DelayDocument7 pagesEarly Identification and Screening: Definition of Developmental Delayadheena simonNo ratings yet
- Knewton Adaptive Learning WhitepaperDocument15 pagesKnewton Adaptive Learning WhitepaperWagane FayeNo ratings yet
- 4f ReflectionDocument1 page4f Reflectionapi-577230763No ratings yet
- Ecocentrism: April 2019Document7 pagesEcocentrism: April 2019Shivam TiwariNo ratings yet
- Approaches To Discourse AnalysisDocument16 pagesApproaches To Discourse AnalysisSaadat Hussain Shahji PanjtaniNo ratings yet
- Module 7 Practical Research DemoDocument12 pagesModule 7 Practical Research DemoMarie TiffanyNo ratings yet
- Zydus Wellnes AR 2019Document213 pagesZydus Wellnes AR 2019ravis1985No ratings yet
- About LG CompanyDocument52 pagesAbout LG CompanyJonna LynneNo ratings yet
- GMAT Critical Reasoning PracticeDocument13 pagesGMAT Critical Reasoning PracticeJananee KumaresanNo ratings yet
- Prospectus21 22Document125 pagesProspectus21 22Vishavjeet Singh GarchaNo ratings yet
- JO - 8 - TOTAL HSE Coordinator InternshipDocument2 pagesJO - 8 - TOTAL HSE Coordinator InternshipudbarryNo ratings yet
- Check List - Product Realisation ProcessDocument4 pagesCheck List - Product Realisation ProcessDisha ShahNo ratings yet
- Department of Education: Narrative Report In-Service Training (INSET) - Day 3Document4 pagesDepartment of Education: Narrative Report In-Service Training (INSET) - Day 3Joven CampuganNo ratings yet
- Residence and Travel Questionnaire: Tataaia/Nb/Dm/126Document2 pagesResidence and Travel Questionnaire: Tataaia/Nb/Dm/126Data CentrumNo ratings yet
- Portfolio Template in Earth ScienceDocument10 pagesPortfolio Template in Earth ScienceAngelica Olasiman EsganaNo ratings yet
- Atlantic Computer: A Bundle of Pricing OptionsDocument36 pagesAtlantic Computer: A Bundle of Pricing OptionsRohit GhoshNo ratings yet
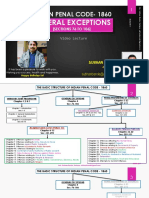
- IPC Part-II PDFDocument38 pagesIPC Part-II PDFHarsh Vardhan Singh HvsNo ratings yet
- Semi-Detailed Lesson Plan in English 7Document2 pagesSemi-Detailed Lesson Plan in English 7Ram Duran82% (11)