You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Clinical Manifestation of Acute Spinal Cord InjuryDocument6 pagesClinical Manifestation of Acute Spinal Cord InjurycpradheepNo ratings yet
- Spinal Cord Injury: Causation & PathophysiologyDocument10 pagesSpinal Cord Injury: Causation & Pathophysiologycpradheep100% (3)
- Spinal Cord BasicsDocument2 pagesSpinal Cord BasicscpradheepNo ratings yet
- Conus Medullaris Vs Cauda Equina SyndromeDocument1 pageConus Medullaris Vs Cauda Equina SyndromecpradheepNo ratings yet
- Clinical Manifestation of Acute Spinal Cord Injury, Chapter-4Document6 pagesClinical Manifestation of Acute Spinal Cord Injury, Chapter-4cpradheepNo ratings yet
- Understanding Girdle Stone ProcedureDocument8 pagesUnderstanding Girdle Stone ProcedurecpradheepNo ratings yet
- Surgical Incisions of Lower LimbDocument11 pagesSurgical Incisions of Lower LimbcpradheepNo ratings yet
- Basic Abdominal ExaminationDocument3 pagesBasic Abdominal Examinationcpradheep100% (1)
- What Is Critical AppraisalDocument8 pagesWhat Is Critical AppraisalcpradheepNo ratings yet
- Conversion Disorder: Background: Conversion Disorder Is Included As A Somatoform DisorderDocument10 pagesConversion Disorder: Background: Conversion Disorder Is Included As A Somatoform Disordercpradheep0% (1)
- Falls Prevention - Safe FootwearDocument1 pageFalls Prevention - Safe FootwearcpradheepNo ratings yet
- Cawthorne Cooksey Vertigo ExercisesDocument1 pageCawthorne Cooksey Vertigo Exercisescpradheep100% (1)
- 6 Minute Walk Test Vs Shuttle Walk TestDocument3 pages6 Minute Walk Test Vs Shuttle Walk TestcpradheepNo ratings yet
- 6 Minute Walk Test ATS GuidelinesDocument7 pages6 Minute Walk Test ATS GuidelinescpradheepNo ratings yet
- Unified Parkinson's Disease Rating Scale (UPDRS)Document5 pagesUnified Parkinson's Disease Rating Scale (UPDRS)cpradheepNo ratings yet
- Spinal Cord Injury Assessment Chart (ASIA)Document2 pagesSpinal Cord Injury Assessment Chart (ASIA)cpradheep100% (5)
- Balance Exercises (Tinetti)Document15 pagesBalance Exercises (Tinetti)cpradheep75% (8)
- Treasure Life.... You Have ONLY OneDocument15 pagesTreasure Life.... You Have ONLY OnecpradheepNo ratings yet
- Innovation in Vascular ClinicDocument22 pagesInnovation in Vascular CliniccpradheepNo ratings yet
- Tracheostomy Care GuidelinesDocument15 pagesTracheostomy Care Guidelinesnurseuragon92% (25)
- Walking Impairment QuestionnairDocument2 pagesWalking Impairment QuestionnaircpradheepNo ratings yet
- Falls Efficacy Scale - International (English)Document1 pageFalls Efficacy Scale - International (English)cpradheep100% (3)
- ABG Flow ChartDocument1 pageABG Flow ChartcpradheepNo ratings yet
- ButterflyDocument11 pagesButterflycpradheepNo ratings yet
- Learning Style / Whats My Learning StyleDocument2 pagesLearning Style / Whats My Learning StylecpradheepNo ratings yet
- 6 Minute Walk Test - Distance CalculatorDocument2 pages6 Minute Walk Test - Distance Calculatorcpradheep100% (2)
- 6 Minute Walk Test InstructionsDocument6 pages6 Minute Walk Test InstructionscpradheepNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
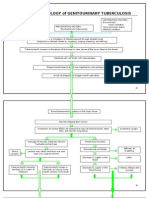
- Pathophysiology of Genitourinary TuberculosisDocument8 pagesPathophysiology of Genitourinary Tuberculosisace_51891No ratings yet
- Chapter 033Document25 pagesChapter 033dtheart2821No ratings yet
- Bladder CancerDocument47 pagesBladder Cancerzeina32100% (1)
- Urinary RetentionDocument11 pagesUrinary RetentionAngga PradianNo ratings yet
- Uti PathoDocument3 pagesUti PathoThrinNo ratings yet
- Session #42 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Document4 pagesSession #42 SAS - AnaPhy (Lab) (Agdana, Nicole Ken)Nicole Ken AgdanaNo ratings yet
- ANS Pharmacology-Cholinergic AgentsDocument55 pagesANS Pharmacology-Cholinergic AgentsMarc Imhotep Cray, M.D.No ratings yet
- Jurnal Urine Drainase ManagementDocument8 pagesJurnal Urine Drainase ManagementSii Silmi DestrianiNo ratings yet
- Urinary Tract Infection (UTI)Document39 pagesUrinary Tract Infection (UTI)Sabita TripathiNo ratings yet
- Peritoneum Omenta Inner HerniasDocument54 pagesPeritoneum Omenta Inner HerniasCatalin SavinNo ratings yet
- NEET PG 2015 Question Paper With SolutionsDocument1,852 pagesNEET PG 2015 Question Paper With SolutionsSK RaulNo ratings yet
- Anatomy ProstateDocument2 pagesAnatomy ProstatenavjavNo ratings yet
- FORMULAS FOR URINARY DIFFICULTY - Dr. Jake Fratkin - Boulder, CODocument5 pagesFORMULAS FOR URINARY DIFFICULTY - Dr. Jake Fratkin - Boulder, COVera Gardasevic MitrovicNo ratings yet
- Ginés Morata: The Excretory SystemDocument3 pagesGinés Morata: The Excretory SystemSonia Navarro FloresNo ratings yet
- Nocturnal Enuresis 021814Document33 pagesNocturnal Enuresis 021814Tanvi ManjrekarNo ratings yet
- Artificial Urinary Sphincter Case ReportDocument12 pagesArtificial Urinary Sphincter Case ReportAaron DesaiNo ratings yet
- Exstrophy-Epispadias Complex: Current Management: Journal ReadingDocument64 pagesExstrophy-Epispadias Complex: Current Management: Journal ReadingAnonymous ce3S6XFdwU100% (1)
- NPR040 Pre-Piped Horizontal Bladder TankDocument6 pagesNPR040 Pre-Piped Horizontal Bladder TankLuis Joel Ramos RamosNo ratings yet
- Fisiologi Genitourinary SystemDocument14 pagesFisiologi Genitourinary SystemPandu Dian WicaksonoNo ratings yet
- CKD (F&e)Document110 pagesCKD (F&e)Al-nazer Azer Al100% (1)
- Urinary System Anatomy and Physiology - Study Guide For Nurses PDFDocument22 pagesUrinary System Anatomy and Physiology - Study Guide For Nurses PDFKhan KhanNo ratings yet
- Urinary Retention After Orthopedic SurgeryDocument3 pagesUrinary Retention After Orthopedic SurgeryJackson HakimNo ratings yet
- Mechanisms, Mitigation, and Management of Urinary Toxicity From Prostate RadiotherapyDocument10 pagesMechanisms, Mitigation, and Management of Urinary Toxicity From Prostate RadiotherapyZuriNo ratings yet
- Gerontological Nursing LectureDocument18 pagesGerontological Nursing Lecturenonalynne8056150% (2)
- GA - Lecture Syllabs Unit2Document55 pagesGA - Lecture Syllabs Unit2محمد خزمهNo ratings yet
- Cystometry "Cystometrogram" (CMG)Document7 pagesCystometry "Cystometrogram" (CMG)Wendy EscalanteNo ratings yet
- Exstrophy of BladderDocument34 pagesExstrophy of BladdersudhiNo ratings yet
- Physiology of MicturitionDocument44 pagesPhysiology of MicturitionEkiran BabajideNo ratings yet
- Urinary SystemDocument10 pagesUrinary SystemMaruen RodriguezNo ratings yet
- Excretion & Osmoregulation: 16. Highlights of This TopicDocument41 pagesExcretion & Osmoregulation: 16. Highlights of This TopicSAGAR PADALKARNo ratings yet