You might also like
- PATHOPHYSIOLOGY of PreeclampsiaDocument1 pagePATHOPHYSIOLOGY of PreeclampsiaPearl IbisateNo ratings yet
- Ectopic Pregnancy PathophysiologyDocument5 pagesEctopic Pregnancy Pathophysiologyjoyrena ochondraNo ratings yet
- Pathophysiology EclampsiaDocument5 pagesPathophysiology EclampsiaYael EzraNo ratings yet
- Pregnancy Induced Hypertension PathophysiologyDocument2 pagesPregnancy Induced Hypertension PathophysiologyCamille Grace100% (1)
- PATHOPHYSIOLOGY - Placenta PreviaDocument5 pagesPATHOPHYSIOLOGY - Placenta PreviaFretzgine Lou Manuel100% (2)
- Iii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsDocument3 pagesIii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsVianne ArcenioNo ratings yet
- Case Study (Preeclampsia)Document6 pagesCase Study (Preeclampsia)Jobelle AcenaNo ratings yet
- PaThoPhysiology of EclampsiaDocument5 pagesPaThoPhysiology of Eclampsiahailleyann100% (2)
- Nursing Process For A Client With Molar Pregnancy (H-Mole)Document24 pagesNursing Process For A Client With Molar Pregnancy (H-Mole)api-370148995% (19)
- Altered Uteroplacental Tissue PerfusionDocument5 pagesAltered Uteroplacental Tissue PerfusionArielle BajalaNo ratings yet
- Normal Spontaneous Vaginal DeliveryDocument35 pagesNormal Spontaneous Vaginal DeliveryJohn Edward EscoteNo ratings yet
- H MoleDocument7 pagesH MoleRaymond Christopher LimNo ratings yet
- Normal Spontaneous Vaginal DeliveryDocument11 pagesNormal Spontaneous Vaginal DeliveryKristine Valenton67% (3)
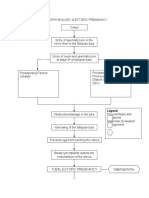
- PATHOPHYSIOLOGY of ECTOPIC PREGNANCYDocument2 pagesPATHOPHYSIOLOGY of ECTOPIC PREGNANCYrye100% (1)
- ABORTION PathophysiologyDocument3 pagesABORTION PathophysiologyChiara FajardoNo ratings yet
- PATHOPHYSIOLOGY MyomaDocument3 pagesPATHOPHYSIOLOGY MyomaDevikomala50% (2)
- Gordon's Functional Health PatternDocument3 pagesGordon's Functional Health PatternDianneNo ratings yet
- Chapter 24: Nursing Care of A Family During A Surgical Intervention For BirthDocument22 pagesChapter 24: Nursing Care of A Family During A Surgical Intervention For BirthAlyssaGrandeMontimorNo ratings yet
- Diagram Myoma IDocument1 pageDiagram Myoma IJoann100% (12)
- Pre EclampsiaDocument13 pagesPre EclampsiaEniamrahs DnalonNo ratings yet
- Myoma PathoniixDocument1 pageMyoma PathoniixRendel FernandezNo ratings yet
- Pathophysiology of Hyperemesis Gravidarum DiagramDocument1 pagePathophysiology of Hyperemesis Gravidarum DiagramQuintin MangaoangNo ratings yet
- After 8 Hours of Nursing Interventions Patient Will Be Able To: Demonstrate Adequate Perfusion. Demonstrate Stable Vital SignsDocument3 pagesAfter 8 Hours of Nursing Interventions Patient Will Be Able To: Demonstrate Adequate Perfusion. Demonstrate Stable Vital Signsroma_elonaNo ratings yet
- Pathophysiology of Ectopic PregnancyDocument1 pagePathophysiology of Ectopic PregnancyLiza MinonaNo ratings yet
- Anatomy Pathophysiology PreeclampsiaDocument4 pagesAnatomy Pathophysiology PreeclampsiaKeith Wesley YbutNo ratings yet
- Pre Eclampsia of Severe FeaturesDocument3 pagesPre Eclampsia of Severe FeaturesPrincess Diane S. VillegasNo ratings yet
- Dilatation and CurettageDocument2 pagesDilatation and CurettageBheru Lal50% (2)
- Managing Abruptio PlacentaDocument29 pagesManaging Abruptio PlacentaAudrey DelfinNo ratings yet
- Incomplete Abortion Case StudyDocument40 pagesIncomplete Abortion Case StudyLani Michelle BelloNo ratings yet
- Nursing Care of Hydatidiform MoleDocument23 pagesNursing Care of Hydatidiform MoleKristel Rivamonte100% (1)
- Nursing Care Plan Abruptio PlacentaeDocument2 pagesNursing Care Plan Abruptio PlacentaeWann WannNo ratings yet
- Problems of the Passageway and Psyche Factors in LaborDocument1 pageProblems of the Passageway and Psyche Factors in LaborAirishNo ratings yet
- Nursing Care Plan for Labor Pain ManagementDocument8 pagesNursing Care Plan for Labor Pain ManagementDickson,Emilia Jade100% (1)
- NCP Abruptio PlacentaDocument2 pagesNCP Abruptio PlacentaCarson Birth100% (1)
- Ectopic PregnancyDocument2 pagesEctopic PregnancyRex Dave Guinoden100% (1)
- H Mole PathoDocument1 pageH Mole PathoKyle AlmeroNo ratings yet
- Hydatidiform MoleDocument2 pagesHydatidiform MoleDaniele Katrina Pimentel100% (3)
- Ovarian Cyst PathophysiologyDocument1 pageOvarian Cyst PathophysiologyShamsa Afdal100% (2)
- NCP Case 3Document3 pagesNCP Case 3boomer SeargeNo ratings yet
- Acute Glomrulonephritis PathophysiologyDocument2 pagesAcute Glomrulonephritis PathophysiologyJai - HoNo ratings yet
- Maternal Risk AssessmentDocument3 pagesMaternal Risk AssessmentMark FernandezNo ratings yet
- Pathophysiology of Uterine FibroidsDocument1 pagePathophysiology of Uterine FibroidsJurilyne Rose TundagNo ratings yet
- Breastfeeding Assessment, Diagnosis, Planning and EvaluationDocument2 pagesBreastfeeding Assessment, Diagnosis, Planning and EvaluationCharmae NaveaNo ratings yet
- CS Case StudyDocument31 pagesCS Case StudyAira MiyaNo ratings yet
- Acute GlomerulonephritisDocument1 pageAcute GlomerulonephritisTaz Bagul MutiNo ratings yet
- Pathophysiology PreeclampsiaDocument1 pagePathophysiology PreeclampsiaPATHOSHOPPENo ratings yet
- Nursing Crib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursing Crib Com NURSING CARE PLAN Spontaneous AbortionJustin PasaronNo ratings yet
- Urinary Tract Infection pATho SHEENADocument2 pagesUrinary Tract Infection pATho SHEENASheena Arnoco ToraynoNo ratings yet
- Nursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionDocument2 pagesNursing Care Plans: Ineffective (Uteroplacental) Tissue PerfusionVincent Paul SantosNo ratings yet
- Pathophysiology NSD FinalDocument2 pagesPathophysiology NSD FinalDaniel Tan Galindez80% (5)
- Nursing Care Plan AbortionDocument4 pagesNursing Care Plan AbortionJane Casiquin100% (1)
- Course in The Ward FinallllllllDocument6 pagesCourse in The Ward FinallllllllJisel-Apple BulanNo ratings yet
- Placenta Previa Case StudyDocument7 pagesPlacenta Previa Case StudyphearlieNo ratings yet
- Nursing Care Plan for Acute Pain ManagementDocument2 pagesNursing Care Plan for Acute Pain Managementjonna casumpangNo ratings yet
- Non Modifiable: Modifiable:: (BP 158/87 MMHG)Document1 pageNon Modifiable: Modifiable:: (BP 158/87 MMHG)Quintin MangaoangNo ratings yet
- Pathophysiology of PreeclampsiaDocument1 pagePathophysiology of PreeclampsiaKristine Alejandro100% (14)
- RLEhospLUMC PATHOPHYSIOLOGYcasepresDocument3 pagesRLEhospLUMC PATHOPHYSIOLOGYcasepresSandy DuranNo ratings yet
- Predisposing Factor Precipitating FactorDocument2 pagesPredisposing Factor Precipitating FactorkamotenikimiNo ratings yet
- Amniotic Fluid EmbolismDocument10 pagesAmniotic Fluid EmbolismRebecca ApeladoNo ratings yet
- Pa Tho ReviseDocument10 pagesPa Tho ReviseCharl SembranoNo ratings yet
- Mari Andrew: Am I There Yet?: The Loop-De-Loop, Zigzagging Journey To AdulthoodDocument4 pagesMari Andrew: Am I There Yet?: The Loop-De-Loop, Zigzagging Journey To Adulthoodjamie carpioNo ratings yet
- Culture and Sensitivity: InhalationDocument3 pagesCulture and Sensitivity: Inhalationjamie carpioNo ratings yet
- Jake - MH TeamDocument1 pageJake - MH Teamjamie carpioNo ratings yet
- Chart 1: The NEWS Scoring System: Physiological Score Parameter 3 2 1 0 1 2 3Document4 pagesChart 1: The NEWS Scoring System: Physiological Score Parameter 3 2 1 0 1 2 3jamie carpio100% (1)
- Cardiovascular Disorders: Types of DysrythmiasDocument3 pagesCardiovascular Disorders: Types of Dysrythmiasjamie carpioNo ratings yet
- Abbey Pain Scale assessment toolDocument2 pagesAbbey Pain Scale assessment toolMuhammad RezgiaNo ratings yet
- Drug Calculations WorkbookDocument32 pagesDrug Calculations Workbookvhon100% (1)
- Brunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 4Document1 pageBrunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 4jamie carpioNo ratings yet
- Brunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 6Document1 pageBrunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 6jamie carpioNo ratings yet
- MUST Malnutrition Universal Screening Tool PDFDocument6 pagesMUST Malnutrition Universal Screening Tool PDFHoria CostrutNo ratings yet
- RowariwudujiladekodazelaDocument3 pagesRowariwudujiladekodazelajamie carpioNo ratings yet
- Public Health Community Health Nursing: Goal: To Enable EveryDocument10 pagesPublic Health Community Health Nursing: Goal: To Enable Everyjamie carpioNo ratings yet
- The ABCDE ApproachDocument8 pagesThe ABCDE ApproachAsmaa TahaNo ratings yet
- Bob Dawson - PhysioDocument1 pageBob Dawson - Physiojamie carpioNo ratings yet
- Jake PetersonDocument1 pageJake Petersonjamie carpioNo ratings yet
- OET Letter FormatDocument8 pagesOET Letter FormatHeba Zaher100% (4)
- Code MNGTDocument3 pagesCode MNGTjamie carpioNo ratings yet
- Writing-General-Information-Tasks (Dragged)Document2 pagesWriting-General-Information-Tasks (Dragged)jamie carpioNo ratings yet
- Artery Bypass GraftDocument3 pagesArtery Bypass GraftJasmine ChuaNo ratings yet
- ABCDs During A Code Blue Response in An Adult PatientDocument23 pagesABCDs During A Code Blue Response in An Adult PatientChakra PuspitaNo ratings yet
- Blood Transfusion and TPN Nursing Care PlansDocument2 pagesBlood Transfusion and TPN Nursing Care Plansjamie carpioNo ratings yet
- Hepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Hepatitis GDocument9 pagesHepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Hepatitis Gjamie carpioNo ratings yet
- OBSTETRICSDocument4 pagesOBSTETRICSjamie carpioNo ratings yet
- Paid Maternity Leave Claiming Personal Exemptions National Immunization DayDocument2 pagesPaid Maternity Leave Claiming Personal Exemptions National Immunization Dayjamie carpioNo ratings yet
- POSITIONSDocument1 pagePOSITIONSjamie carpioNo ratings yet
- Ra 07305 FVR PDFDocument11 pagesRa 07305 FVR PDFjamie carpioNo ratings yet
- MS TopicsDocument1 pageMS Topicsjamie carpioNo ratings yet
- CONCEPTSDocument1 pageCONCEPTSjamie carpioNo ratings yet
- Rapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of LifeDocument8 pagesRapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of Lifejamie carpioNo ratings yet
- EBP Implementation Leadership of Frontline Nurse Managers: Validation of The Implementation Leadership Scale in Acute CareDocument10 pagesEBP Implementation Leadership of Frontline Nurse Managers: Validation of The Implementation Leadership Scale in Acute Carejamie carpioNo ratings yet
- Chapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusDocument10 pagesChapter 13 - Diseases of White Blood Cells, Lymph Nodes, Spleen, and ThymusAgnieszka WisniewskaNo ratings yet
- Sunidhi Final PrintDocument79 pagesSunidhi Final PrintrthrthgNo ratings yet
- Short Medical Abbreviations ListDocument22 pagesShort Medical Abbreviations ListrastikadewiNo ratings yet
- New Updates To Congestive Heart Failure PPT INTDocument75 pagesNew Updates To Congestive Heart Failure PPT INTSiqki PerryNo ratings yet
- Ischemic Stroke Case SummaryDocument31 pagesIschemic Stroke Case SummaryHariniNo ratings yet
- Abnoramal ECGDocument20 pagesAbnoramal ECGImmanuelNo ratings yet
- Innervation and Vascularization of Head and NeckDocument36 pagesInnervation and Vascularization of Head and NeckDrgDondyNo ratings yet
- COPD PathoDocument1 pageCOPD PathoLeah May AnchetaNo ratings yet
- Important Repeatedly Asked QuestionsDocument5 pagesImportant Repeatedly Asked QuestionsAbey GeorgeNo ratings yet
- Kidney Disease Diagnosis and Management GuideDocument5 pagesKidney Disease Diagnosis and Management GuideJerin XavierNo ratings yet
- RH Isoimmunization DR SamiraDocument37 pagesRH Isoimmunization DR Samiragynaecology2010100% (2)
- Hiv 1Document103 pagesHiv 1dhwanit31No ratings yet
- Safe and Unsafe Drugs During PregnancyDocument12 pagesSafe and Unsafe Drugs During PregnancyfirdaustheshadowNo ratings yet
- DEAR TO NCLEX's HEART PDFDocument452 pagesDEAR TO NCLEX's HEART PDFrn msn100% (4)
- 2009-Giardiasis - Why Do The Symptoms Sometimes Never StopDocument8 pages2009-Giardiasis - Why Do The Symptoms Sometimes Never StopwiwienNo ratings yet
- Parkinson's DiseaseDocument51 pagesParkinson's DiseaseNinz Taruc0% (1)
- MRCP UK PACES EXAM GUIDEDocument124 pagesMRCP UK PACES EXAM GUIDEJayachandran P KNo ratings yet
- Medical Semiology MCQS AnswersDocument12 pagesMedical Semiology MCQS AnswersMINANI Theobald80% (5)
- Unilateral Lower Limb SwellingDocument1 pageUnilateral Lower Limb SwellingLilius TangNo ratings yet
- 2015 To 2019 Super Speciality Dissertation Topics PDFDocument35 pages2015 To 2019 Super Speciality Dissertation Topics PDFJoseph John Crasto100% (3)
- Trusted Medical Answers-In Seconds.: Lipid DisordersDocument13 pagesTrusted Medical Answers-In Seconds.: Lipid DisordersMohammed shamiul Shahid100% (1)
- ICU One Pager Lactic Acidosis-Zxle8yDocument1 pageICU One Pager Lactic Acidosis-Zxle8yhanady alsnedNo ratings yet
- 4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFDocument89 pages4.15 DR. ROBERTO MIRASOL HYperthyroidism PSEM 2017 1 PDFjackie funtanilla100% (1)
- Targeted Therapy for Bone, Joint and Soft Tissue TumorsDocument37 pagesTargeted Therapy for Bone, Joint and Soft Tissue Tumorsputri aisheNo ratings yet
- NCM 106 Rle Module 2Document26 pagesNCM 106 Rle Module 2Esmareldah Henry SirueNo ratings yet
- CoccocidiopsisDocument10 pagesCoccocidiopsisMoises PinedaNo ratings yet
- Haad Exam McqsDocument727 pagesHaad Exam McqsSadafRafiNadeemNo ratings yet
- OBAT ANTI-DIABETES - Hernita - 2019Document70 pagesOBAT ANTI-DIABETES - Hernita - 2019Hernita TaurustyaNo ratings yet
- Tamsulosin Dosage, Adverse Effects and Nursing ConsiderationsDocument9 pagesTamsulosin Dosage, Adverse Effects and Nursing ConsiderationsChristine BorromeoNo ratings yet