You might also like
- Professional Disclosure StatementDocument2 pagesProfessional Disclosure Statementapi-253915117100% (2)
- Acp Module 5Document32 pagesAcp Module 5Mechel Cabaltera87% (15)
- Professional Counseling Disclosure StatementDocument2 pagesProfessional Counseling Disclosure Statementapi-234763514100% (1)
- Professional Disclosure Statement and Informed Consent 2Document3 pagesProfessional Disclosure Statement and Informed Consent 2api-253782185No ratings yet
- The Devil and the Dark Water: A Locked-Room Historical MysteryFrom EverandThe Devil and the Dark Water: A Locked-Room Historical MysteryRating: 3.5 out of 5 stars3.5/5 (303)
- The Big Four: A Hercule Poirot MysteryFrom EverandThe Big Four: A Hercule Poirot MysteryRating: 3.5 out of 5 stars3.5/5 (747)
- Professional Disclosure Statement S ValentineDocument2 pagesProfessional Disclosure Statement S Valentineapi-316614503No ratings yet
- SchoolpdsDocument2 pagesSchoolpdsapi-307653540No ratings yet
- Lpca Professional Disclosure Statement Mann 2015Document3 pagesLpca Professional Disclosure Statement Mann 2015api-301673059100% (1)
- Professional Disclosure Statement Updated 2016Document2 pagesProfessional Disclosure Statement Updated 2016api-337285911No ratings yet
- The Murder of Roger Ackroyd: A Hercule Poirot MysteryFrom EverandThe Murder of Roger Ackroyd: A Hercule Poirot MysteryRating: 4 out of 5 stars4/5 (2453)
- A Shot in the Dark: A Constable Twitten MysteryFrom EverandA Shot in the Dark: A Constable Twitten MysteryRating: 3.5 out of 5 stars3.5/5 (61)
- Sidney Chambers and The Shadow of Death: Grantchester Mysteries 1From EverandSidney Chambers and The Shadow of Death: Grantchester Mysteries 1Rating: 3.5 out of 5 stars3.5/5 (262)
- The Divine Private Detective Agency Collection: Sister Eve, Private Eye, The Case of the Sin City Sister, Sister Eve and the Blue NunFrom EverandThe Divine Private Detective Agency Collection: Sister Eve, Private Eye, The Case of the Sin City Sister, Sister Eve and the Blue NunRating: 3.5 out of 5 stars3.5/5 (30)
- Poirot Investigates: 30 Cases of the Most Famous Belgian Detective - Murder Mystery Boxed Set: The Murder of Roger Ackroyd, The Mysterious Affair at Styles, The Murder on the Link...sFrom EverandPoirot Investigates: 30 Cases of the Most Famous Belgian Detective - Murder Mystery Boxed Set: The Murder of Roger Ackroyd, The Mysterious Affair at Styles, The Murder on the Link...sNo ratings yet
- The Arly Hanks Mysteries Volume One: Malice in Maggody, Mischief in Maggody, and Much Ado in MaggodyFrom EverandThe Arly Hanks Mysteries Volume One: Malice in Maggody, Mischief in Maggody, and Much Ado in MaggodyRating: 4.5 out of 5 stars4.5/5 (3)
- Sidney Chambers and The Persistence of Love: Grantchester Mysteries 6From EverandSidney Chambers and The Persistence of Love: Grantchester Mysteries 6Rating: 3.5 out of 5 stars3.5/5 (34)
- Pds UpdatedDocument2 pagesPds Updatedapi-609488951No ratings yet
- Professional Disclosure 2014Document3 pagesProfessional Disclosure 2014api-258381393No ratings yet
- Professional Disclosure StatementDocument3 pagesProfessional Disclosure Statementapi-642170591No ratings yet
- Ads Professionaldisclosurestatement Fall 2021 2Document3 pagesAds Professionaldisclosurestatement Fall 2021 2api-582911813No ratings yet
- Professional Disclosure StatementDocument2 pagesProfessional Disclosure Statementapi-316348538No ratings yet
- Pds Capstone 5 April 2023Document2 pagesPds Capstone 5 April 2023api-663797542No ratings yet
- Professional Disclosure Statement 6 2016 For WeeblyDocument3 pagesProfessional Disclosure Statement 6 2016 For Weeblyapi-314123316No ratings yet
- Ananya Ranjan Disclosure Statement-1Document3 pagesAnanya Ranjan Disclosure Statement-1api-664529975No ratings yet
- Professional Disclosure Statement FinalDocument6 pagesProfessional Disclosure Statement Finalapi-661682802No ratings yet
- Sophie Young Eportfolio Pds 2022Document2 pagesSophie Young Eportfolio Pds 2022api-609422028No ratings yet
- Professional Disclosure Statement UpdatedDocument2 pagesProfessional Disclosure Statement Updatedapi-326282879No ratings yet
- Professional Disclosure Statement LcmhcaDocument5 pagesProfessional Disclosure Statement Lcmhcaapi-664373899No ratings yet
- White Professional Disclosure StatementDocument2 pagesWhite Professional Disclosure Statementapi-292469278No ratings yet
- Rachel Carter Professional Disclosure StatementDocument5 pagesRachel Carter Professional Disclosure Statementapi-352566916No ratings yet
- Professional Disclosure StatementDocument4 pagesProfessional Disclosure Statementapi-710318288No ratings yet
- Professional Counseling ConsentDocument3 pagesProfessional Counseling ConsentBLAST REHANNo ratings yet
- Lpca Professional Disclosure StatementDocument2 pagesLpca Professional Disclosure Statementapi-417127832No ratings yet
- Memory Counseling Program Medical Center Boulevard Winston-Salem, NC 27157 Phone: 336-716-1034Document4 pagesMemory Counseling Program Medical Center Boulevard Winston-Salem, NC 27157 Phone: 336-716-1034api-356736216No ratings yet
- Disclosure Statement FinalDocument2 pagesDisclosure Statement Finalapi-223922718No ratings yet
- Professional Disclosure Statement For Jenny Buysse Counseling and Career ConsultingDocument4 pagesProfessional Disclosure Statement For Jenny Buysse Counseling and Career Consultingapi-357648039No ratings yet
- Professional Disclosure and Informed Consent Kristi MDocument3 pagesProfessional Disclosure and Informed Consent Kristi MArely AguilarNo ratings yet
- Professional Disclosure StatementDocument2 pagesProfessional Disclosure Statementapi-309973906No ratings yet
- PdstemplateDocument3 pagesPdstemplateapi-531337210No ratings yet
- Central Information Commission: Prof. M. Sridhar Acharyulu (Madabhushi Sridhar)Document11 pagesCentral Information Commission: Prof. M. Sridhar Acharyulu (Madabhushi Sridhar)venugopal murthyNo ratings yet
- Chapter 2Document8 pagesChapter 2Zyrome Jen HarderNo ratings yet
- (Models and Modeling in Science Education 4) John K. Gilbert, David F. Treagust (Auth.), Prof. John K. Gilbert, Prof. David Treagust (Eds.)-Multiple Representations in Chemical Education-Springer Neth (Recovered)Document369 pages(Models and Modeling in Science Education 4) John K. Gilbert, David F. Treagust (Auth.), Prof. John K. Gilbert, Prof. David Treagust (Eds.)-Multiple Representations in Chemical Education-Springer Neth (Recovered)NestiNo ratings yet
- Instructions Below For Junior College Registration FormDocument4 pagesInstructions Below For Junior College Registration FormShaikh WasimaNo ratings yet
- Department OF Education: Director IVDocument2 pagesDepartment OF Education: Director IVApril Mae ArcayaNo ratings yet
- CyberparkHoldings Inc.Document22 pagesCyberparkHoldings Inc.Homer SebastianNo ratings yet
- Context, Conditions, and CultureDocument5 pagesContext, Conditions, and CultureOnaizaNo ratings yet
- Untitled DocumentDocument8 pagesUntitled DocumentAkshat PagareNo ratings yet
- A2 BSBLDR402 Lead Effec Workplace Rel-UpdatedDocument8 pagesA2 BSBLDR402 Lead Effec Workplace Rel-Updatedmanish gurungNo ratings yet
- Topic 2 Guidance and Counselling For ChildrenDocument30 pagesTopic 2 Guidance and Counselling For Childrenlky411No ratings yet
- Chuyen de 2 - Quyen Luc Va Su Anh HuongDocument27 pagesChuyen de 2 - Quyen Luc Va Su Anh HuongThảo NgânNo ratings yet
- Fundamentals of BioethicsDocument14 pagesFundamentals of BioethicsJonah R. MeranoNo ratings yet
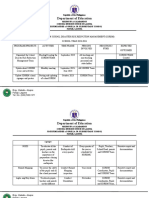
- SDRRM Action Plan 2023-2024Document3 pagesSDRRM Action Plan 2023-2024Lerma EmNo ratings yet
- WHLP WEEK 7 Quarter 2 IMPDocument8 pagesWHLP WEEK 7 Quarter 2 IMPDarwin Ladiero Morales LptNo ratings yet
- Mil Summative Quiz 1 CompleteDocument2 pagesMil Summative Quiz 1 CompleteEverdina GiltendezNo ratings yet
- MPA - Kakiziba, Christina - 2015 PDFDocument79 pagesMPA - Kakiziba, Christina - 2015 PDFHumphrey UrlandaNo ratings yet
- Understanding The Self: Module 1 Contents/ LessonsDocument6 pagesUnderstanding The Self: Module 1 Contents/ LessonsGuki Suzuki100% (6)
- Syllabus Advanced Cad Cam Spring 2013Document6 pagesSyllabus Advanced Cad Cam Spring 2013api-236166548No ratings yet
- Personal Space Lesson PlanDocument5 pagesPersonal Space Lesson Planapi-392223990No ratings yet
- 8th Grade Georgia Studies Multiple Choice Assessment New South Era Standard SS8H7Document11 pages8th Grade Georgia Studies Multiple Choice Assessment New South Era Standard SS8H7Shawn DaviesNo ratings yet
- Arrays GameDocument2 pagesArrays Gameapi-311154509No ratings yet
- 1 Education Confined To Educational Institutions IsDocument4 pages1 Education Confined To Educational Institutions IsAndeel RanaNo ratings yet
- Intellect's New 2013 Journal CatalogueDocument37 pagesIntellect's New 2013 Journal CatalogueIntellect BooksNo ratings yet
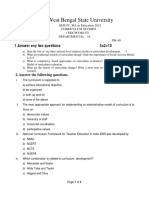
- West Bengal State University: 1.answer Any Two Questions: 5x2 10Document3 pagesWest Bengal State University: 1.answer Any Two Questions: 5x2 10Cracked English with Diganta RoyNo ratings yet
- E SAT - Final.schoolheads.2019Document15 pagesE SAT - Final.schoolheads.2019Manuelito MontoyaNo ratings yet
- PGD Brochure 10th BatchDocument13 pagesPGD Brochure 10th BatchSaiful Islam PatwaryNo ratings yet
- Baseline Assessment Worldbank PDFDocument134 pagesBaseline Assessment Worldbank PDFYvi RozNo ratings yet
- Cross Cultural Misunderstandings LessonDocument3 pagesCross Cultural Misunderstandings LessonAna Fe0% (1)
- Discover The 6 Qualities of The 21st Century TeacherDocument31 pagesDiscover The 6 Qualities of The 21st Century TeacherTomas DocaNo ratings yet