You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Running Head: Go-Row Paddle System 1Document12 pagesRunning Head: Go-Row Paddle System 1api-292815157No ratings yet
- Trans PTTDocument43 pagesTrans PTTapi-292815157100% (1)
- Social Justice ReflectionDocument2 pagesSocial Justice Reflectionapi-292815157No ratings yet
- CatevidencetableworksheetDocument40 pagesCatevidencetableworksheetapi-292815157No ratings yet
- Hospice FW EvalDocument6 pagesHospice FW Evalapi-292815157No ratings yet
- FW EvalDocument6 pagesFW Evalapi-292815157No ratings yet
- Occupational Profile AnalysisDocument20 pagesOccupational Profile Analysisapi-292815157No ratings yet
- Sup PaperDocument12 pagesSup Paperapi-292815157No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Investigation of The Phenomenon of Propagated Sensation Along The Channels in The Upper Limb Following Administration of Acupuncture and Mock LaserDocument10 pagesInvestigation of The Phenomenon of Propagated Sensation Along The Channels in The Upper Limb Following Administration of Acupuncture and Mock LaserSebastiano SerraNo ratings yet
- Lecture 2, Methods of Measuring Oral DiseasesDocument4 pagesLecture 2, Methods of Measuring Oral DiseasesJustDen09100% (1)
- Juvenile Giant Fibroadenoma Presenting in 12 Years Old Girl, A Rare Presentation With Review of LiteratureDocument3 pagesJuvenile Giant Fibroadenoma Presenting in 12 Years Old Girl, A Rare Presentation With Review of LiteratureIOSRjournalNo ratings yet
- Herbalist and Alchemist Books: Catalog #48Document20 pagesHerbalist and Alchemist Books: Catalog #48corbu_georgeNo ratings yet
- LAPORAN KASUS Sol IntracranialDocument96 pagesLAPORAN KASUS Sol IntracranialJessica FilbertineNo ratings yet
- StonaDocument29 pagesStonapoonam seeptungNo ratings yet
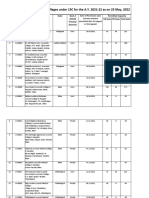
- List of Permitted Ayurveda Colleges For The A.Y. 2021-22 Till 06.05.2022Document52 pagesList of Permitted Ayurveda Colleges For The A.Y. 2021-22 Till 06.05.2022Re Ed EstNo ratings yet
- AnxietyDocument23 pagesAnxietyJanette DickersonNo ratings yet
- Lymphatic System and San JiaoDocument6 pagesLymphatic System and San JiaoΒιβιλάκη Γεωργία100% (1)
- Red Flags of The Shoulder and NeckDocument5 pagesRed Flags of The Shoulder and NecksugoimanNo ratings yet
- Cardiogenic ShockDocument18 pagesCardiogenic ShockBagus Andi PramonoNo ratings yet
- 2005 ProactiveDocument11 pages2005 ProactiveBanky SupittayapornNo ratings yet
- Base Excess The BasicsDocument7 pagesBase Excess The BasicsStaporn KasemsripitakNo ratings yet
- Approved Practice Setting With Facility License Number and Contact Oct 2023Document30 pagesApproved Practice Setting With Facility License Number and Contact Oct 2023ns5qp4t26dNo ratings yet
- When Panic Attacks - Module 1 - Overview of PanicDocument9 pagesWhen Panic Attacks - Module 1 - Overview of PaniccatherinekellymuscatNo ratings yet
- Janis & Feshback (1953)Document15 pagesJanis & Feshback (1953)Stephanie LynchNo ratings yet
- Philippine Journal of Child Sexual AbuseDocument17 pagesPhilippine Journal of Child Sexual AbuseHector MasonNo ratings yet
- Niromathe Book en PDFDocument102 pagesNiromathe Book en PDFChibulcutean0% (1)
- Life Mapping Templates v1Document4 pagesLife Mapping Templates v1Maria Mastroianni100% (1)
- V680 FSN Removal Letter UPDATE 27JUL2023 - SignedDocument6 pagesV680 FSN Removal Letter UPDATE 27JUL2023 - SignedsrinibmeNo ratings yet
- Cms 2567 05-13-08Document41 pagesCms 2567 05-13-08jawtrey100% (3)
- Nursing Care Plan (Post Op Exlap)Document2 pagesNursing Care Plan (Post Op Exlap)Kay D. BeredoNo ratings yet
- Modul 06 PDFDocument16 pagesModul 06 PDFL TereNo ratings yet
- CHAPTER 9 HomeworkDocument5 pagesCHAPTER 9 HomeworkSaravanan SaravanankNo ratings yet
- 6.monitoring in AnesthesiaDocument46 pages6.monitoring in AnesthesiaIlham rianda100% (5)
- Magnesium Sulphate Flash CardsDocument3 pagesMagnesium Sulphate Flash CardsNik AminNo ratings yet
- Mls2f Activity 12 and 13 Gonzaga, Halamane, GilayDocument26 pagesMls2f Activity 12 and 13 Gonzaga, Halamane, GilayBeatriz GonzagaNo ratings yet
- Vitamin KDocument3 pagesVitamin KnaraNo ratings yet
- CBCDocument12 pagesCBCDaNa Al-jomah100% (1)
- Fistula PerianalDocument25 pagesFistula PerianalHafiizh Dwi PramuditoNo ratings yet