You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Biochemistry: SMASHUSMLE Biochemistry Lecture NotesDocument40 pagesBiochemistry: SMASHUSMLE Biochemistry Lecture NotesRaju NiraulaNo ratings yet
- Adenoviruses ParvovirusesDocument74 pagesAdenoviruses ParvovirusesMohammad AlHamdanyNo ratings yet
- Endocrinology: Byu Pdbio 305 Dr. Rhees EndocrinologyDocument8 pagesEndocrinology: Byu Pdbio 305 Dr. Rhees EndocrinologyMohammad AlHamdanyNo ratings yet
- Neeraj CS NotesDocument27 pagesNeeraj CS NotesRohi Afa100% (1)
- 18 9Document15 pages18 9Mohammad AlHamdanyNo ratings yet
- Syllabus in PsychiatryDocument7 pagesSyllabus in PsychiatryMohammad AlHamdanyNo ratings yet
- TEAM Student Manual 2nd Edition For The CDDocument128 pagesTEAM Student Manual 2nd Edition For The CDMohammad AlHamdanyNo ratings yet
- USMLE STEP 1 and STEP 2 Highly Tested Topics Gold CollectionDocument36 pagesUSMLE STEP 1 and STEP 2 Highly Tested Topics Gold CollectionTyler Lawrence CoyeNo ratings yet
- Handling Questions Step by Step by Steven R. Daugherty, PH.D PDFDocument4 pagesHandling Questions Step by Step by Steven R. Daugherty, PH.D PDFYossef HammamNo ratings yet
- Disorders of PerceptionDocument14 pagesDisorders of PerceptionMohammad AlHamdanyNo ratings yet
- Handout+Step+2+OB+Sakala+Jan+2014.ppt4+ (1) - Part 1 PDFDocument11 pagesHandout+Step+2+OB+Sakala+Jan+2014.ppt4+ (1) - Part 1 PDFMohammad AlHamdany100% (2)
- Chapter 18 Metabolic Pathways and Energy Production: 18.2 Digestion: Stage 1Document8 pagesChapter 18 Metabolic Pathways and Energy Production: 18.2 Digestion: Stage 1Mohammad AlHamdanyNo ratings yet
- Biostatistics - Descriptive StatDocument34 pagesBiostatistics - Descriptive StatMohammad AlHamdanyNo ratings yet
- Lection 1Document62 pagesLection 1Mohammad AlHamdanyNo ratings yet
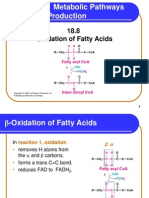
- Chapter 18 Metabolic Pathways and Energy Production: 18.8 Oxidation of Fatty AcidsDocument20 pagesChapter 18 Metabolic Pathways and Energy Production: 18.8 Oxidation of Fatty AcidsMohammad AlHamdanyNo ratings yet
- 18 6Document22 pages18 6Mohammad AlHamdanyNo ratings yet
- He Ma To PoiesisDocument35 pagesHe Ma To PoiesisMohammad AlHamdanyNo ratings yet
- Chapter 17 Nucleic Acids and Protein SynthesisDocument46 pagesChapter 17 Nucleic Acids and Protein SynthesisMohammad AlHamdanyNo ratings yet
- 5 Common Chemical Reaction Types ExplainedDocument18 pages5 Common Chemical Reaction Types ExplainedMohammad AlHamdany100% (1)
- The Adrenal Gland: Anatomy and Hormone ProductionDocument28 pagesThe Adrenal Gland: Anatomy and Hormone ProductionMona NasrNo ratings yet
- Chapter 18 Metabolic Pathways and Energy ProductionDocument13 pagesChapter 18 Metabolic Pathways and Energy ProductionMohammad AlHamdanyNo ratings yet
- Haemo PoiesisDocument29 pagesHaemo PoiesisMohammad AlHamdanyNo ratings yet
- Anatomy Lecture 1Document28 pagesAnatomy Lecture 1Mohammad AlHamdanyNo ratings yet
- Anatomy Lecture 1Document28 pagesAnatomy Lecture 1Mohammad AlHamdanyNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Summary of Endocrine DisordersDocument2 pagesSummary of Endocrine DisordersKrysny MontebonNo ratings yet
- MSD High Risk Medications Inpatient SettingDocument49 pagesMSD High Risk Medications Inpatient SettingAGUSTINA KNo ratings yet
- Correlation of Hyperglycemia With Mortality After Acute Ischemic StrokeDocument8 pagesCorrelation of Hyperglycemia With Mortality After Acute Ischemic Strokeamad markaNo ratings yet
- Impact of Surgical Nutrition on Patient OutcomesDocument54 pagesImpact of Surgical Nutrition on Patient OutcomesAmir SharifNo ratings yet
- 06nov Dec Sf2Document14 pages06nov Dec Sf2freemedicNo ratings yet
- Diabetus MellitusDocument74 pagesDiabetus MellitusVincent SerNo ratings yet
- Pediatric Head Trauma: Yana Puckett, MDDocument37 pagesPediatric Head Trauma: Yana Puckett, MDANUSIBINo ratings yet
- CS20 SolvedDocument2 pagesCS20 SolvedgogoNo ratings yet
- Chronic Complications of Diabetes: Retinopathy, Nephropathy, NeuropathyDocument48 pagesChronic Complications of Diabetes: Retinopathy, Nephropathy, NeuropathyReina TarihoranNo ratings yet
- Meglitinides ProjectDocument10 pagesMeglitinides Projectarmaan kaltaNo ratings yet
- Diabetes GuidelinesDocument29 pagesDiabetes GuidelinesFabiola NogaNo ratings yet
- Unstable Blood GlucoseDocument6 pagesUnstable Blood Glucosetherese BNo ratings yet
- Pass Critical Care Endocrine Frcem ResourcesDocument41 pagesPass Critical Care Endocrine Frcem ResourcesYoussef SaadNo ratings yet
- Ispad 2022Document477 pagesIspad 2022hakimadnenNo ratings yet
- Diabetic Emergencies During Ramadan FastingDocument4 pagesDiabetic Emergencies During Ramadan FastingAmany SalamaNo ratings yet
- Proceeding Book 28th Jakarta Diabates Meeting 2019Document19 pagesProceeding Book 28th Jakarta Diabates Meeting 2019David DwiputeraNo ratings yet
- Comp - Appraisal Pre Final Assignment 2Document32 pagesComp - Appraisal Pre Final Assignment 2Joanne Bernadette AguilarNo ratings yet
- World Journal of Oral and Maxillofacial SurgeryDocument4 pagesWorld Journal of Oral and Maxillofacial SurgeryRemedyPublication3No ratings yet
- Weaknes S/ Fatigue Polyphag IaDocument5 pagesWeaknes S/ Fatigue Polyphag IaEwert Hesketh Nillama PaquinganNo ratings yet
- The Bioartificial Pancreas (BAP)Document16 pagesThe Bioartificial Pancreas (BAP)Madalina FleancuNo ratings yet
- Brunner Answer KeyDocument13 pagesBrunner Answer KeyMaria Luisa Villaluna100% (2)
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDocument1 pageSteroid Tapering and Supportive Treatment Guidance V1.0 PDFPatricia MaisekaNo ratings yet
- NCP: Diabetes Mellitus Prepregnancy/GestationalDocument11 pagesNCP: Diabetes Mellitus Prepregnancy/GestationalJavie85% (13)
- Antidiabetic Drugs. Nurse 2024Document32 pagesAntidiabetic Drugs. Nurse 2024Ayro Business CenterNo ratings yet
- Carbohydrates SummaryDocument9 pagesCarbohydrates SummaryHarold NagunaNo ratings yet
- Anti-Diabetic Effects of Mani-Manian LeavesDocument7 pagesAnti-Diabetic Effects of Mani-Manian Leaveselieza salvadorNo ratings yet
- FnE MCQsDocument11 pagesFnE MCQsGladys YaresNo ratings yet
- Sample Doctor Letter From Practical Diabetology PDFDocument1 pageSample Doctor Letter From Practical Diabetology PDFPainNo ratings yet
- CC - DAY 2 - PRE-TEST RationalizationDocument30 pagesCC - DAY 2 - PRE-TEST RationalizationVincent AmitNo ratings yet
- Journal A. Arviani Desianti NurDocument9 pagesJournal A. Arviani Desianti NurPengetikan ARVNo ratings yet