You might also like
- Ileal Conduit Obstruction EvaluationDocument17 pagesIleal Conduit Obstruction Evaluationkhushi786No ratings yet
- Bile Leakage During Laparoscopic Cholecystectomy A Rare Case of Aberrant AnatomyDocument6 pagesBile Leakage During Laparoscopic Cholecystectomy A Rare Case of Aberrant AnatomyEditor IJTSRDNo ratings yet
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedNo ratings yet
- Powerpoint: Liver Surgical DiseasesDocument95 pagesPowerpoint: Liver Surgical Diseasesj.doe.hex_8792% (12)
- Biliary SystemDocument83 pagesBiliary SystemeviltohuntNo ratings yet
- Surgical Management of Benign Causes of Obstructive JaundiceDocument29 pagesSurgical Management of Benign Causes of Obstructive JaundiceNaviNo ratings yet
- CT AbdomDocument1 pageCT AbdomifeanyiNo ratings yet
- Iatrogenci BDIDocument90 pagesIatrogenci BDIUsmle GuyNo ratings yet
- Hartley Final PDFDocument16 pagesHartley Final PDFAlexandriaJoNo ratings yet
- Topic 23. X-RayDocument2 pagesTopic 23. X-RayMadeline WanhartNo ratings yet
- KDI306 - L34 Tramed BOF - IVUDocument93 pagesKDI306 - L34 Tramed BOF - IVUYodi SoebadiNo ratings yet
- Surgical resection for gallstone ileus and abscessDocument2 pagesSurgical resection for gallstone ileus and abscessMartin WongNo ratings yet
- All About The IVP: April 1 2004 Andrea WilsonDocument30 pagesAll About The IVP: April 1 2004 Andrea WilsonCory Monica MarpaungNo ratings yet
- EMERGENCY DUTY REPORTDocument46 pagesEMERGENCY DUTY REPORTAldo Febriananto KurniawanNo ratings yet
- Cholecystectomy Iatrogenic Bile Duct Injury: April 28, 2005 OHSU, Department of Diagnostic Radiology Kan Hwee, MS4Document35 pagesCholecystectomy Iatrogenic Bile Duct Injury: April 28, 2005 OHSU, Department of Diagnostic Radiology Kan Hwee, MS4SahirNo ratings yet
- Sur - Atlas of Gastrointestinal Surgery (Cameron) NewDocument474 pagesSur - Atlas of Gastrointestinal Surgery (Cameron) Newalisolouki40100% (12)
- Urinary DiversionDocument44 pagesUrinary Diversionminnalesri100% (1)
- Variations in the arterial supply to the gallbladder and critical view of safetyDocument3 pagesVariations in the arterial supply to the gallbladder and critical view of safetyDeni Marie GomonidNo ratings yet
- Kub IvpDocument46 pagesKub IvpBryJos tiongsonNo ratings yet
- 10 KidneysDocument6 pages10 KidneysMark PadulloNo ratings yet
- Live Course Handout - CFMDocument39 pagesLive Course Handout - CFMDrMohamed Elsonosy100% (1)
- Gallbladder and Extrahepatic Biliary System - FinlDocument14 pagesGallbladder and Extrahepatic Biliary System - FinlJoevet T. TadlasNo ratings yet
- CholecystectomyDocument9 pagesCholecystectomyAmyandNo ratings yet
- Barium Follow-Through TBLDocument16 pagesBarium Follow-Through TBLKyo Jie Ming100% (1)
- The Gallbladder Diseases Bile Duct StoneDocument69 pagesThe Gallbladder Diseases Bile Duct Stoneحميد حيدرNo ratings yet
- Intestinal ObstructionDocument52 pagesIntestinal ObstructionAsfandyar Khan100% (2)
- Radiology Imaging of Urinary TractDocument40 pagesRadiology Imaging of Urinary TractMuhammad Zaniar RamadhaniNo ratings yet
- Hepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyDocument4 pagesHepatic Subcapsular BIloma A Rare Complication of Laparoscopic CholecystectomyIndra PrimaNo ratings yet
- Post LapChole Bile LeaksDocument41 pagesPost LapChole Bile LeaksIfeanyichukwu OgbonnayaNo ratings yet
- Management of Accessory Hepatic Ducts in Choledochal CystsDocument2 pagesManagement of Accessory Hepatic Ducts in Choledochal CystsJosé MartínezNo ratings yet
- Chapter 32 Gallbladder and The Extrahepatic Biliary SystemDocument81 pagesChapter 32 Gallbladder and The Extrahepatic Biliary SystemAlexious Marie Callueng100% (1)
- Bile Leaks After Laparoscopic CholecystectomyDocument25 pagesBile Leaks After Laparoscopic CholecystectomyPinky NairNo ratings yet
- CHOLECYSTECTOMYDocument6 pagesCHOLECYSTECTOMYJagannath DasNo ratings yet
- BiliaryDocument41 pagesBiliaryayundyawibowoNo ratings yet
- Surgery OSPEDocument86 pagesSurgery OSPEBrave LionNo ratings yet
- LiverDocument25 pagesLiverVainatheya AnanthNo ratings yet
- Hep Resxn TechDocument33 pagesHep Resxn TechKartikKulshresthaNo ratings yet
- Radiology Emergency: by Dr. Edwin Hasiholan Pandjaitan, SpradDocument72 pagesRadiology Emergency: by Dr. Edwin Hasiholan Pandjaitan, SpradTiara AlexanderNo ratings yet
- Acute AbdomenDocument73 pagesAcute AbdomenWahyu DustnamNo ratings yet
- GI BileDuct ProtocolDocument9 pagesGI BileDuct ProtocolElloide PajutanNo ratings yet
- Kuliah Blok GI Tract - USG Abd - September 2010Document65 pagesKuliah Blok GI Tract - USG Abd - September 2010Natallia BatuwaelNo ratings yet
- LDLTDocument35 pagesLDLTshruthirangan0706No ratings yet
- CT Abdomen - Hosiana O W - 42180258Document18 pagesCT Abdomen - Hosiana O W - 42180258HOSIANAOWNo ratings yet
- Hot GatesDocument38 pagesHot GatesGeorge Mihail ManNo ratings yet
- Nasser2015Document5 pagesNasser2015hengkileonardNo ratings yet
- Ureteritis Cystica Causing ObstructionDocument2 pagesUreteritis Cystica Causing ObstructionDeba P SarmaNo ratings yet
- Ureteroneocystostomy For Treatment of Struvite UroDocument4 pagesUreteroneocystostomy For Treatment of Struvite UroBright DerlacuzENo ratings yet
- Suci TmboDocument15 pagesSuci TmboyongkyNo ratings yet
- Lap Chole DictationDocument2 pagesLap Chole DictationAshish DongreNo ratings yet
- Surgery BoardsDocument16 pagesSurgery Boardscusom34100% (1)
- D2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologyDocument66 pagesD2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologySuneel Kaushik KNo ratings yet
- DitoooongDocument8 pagesDitoooongAkreditasi Sungai AbangNo ratings yet
- (03241750 - Acta Medica Bulgarica) Horseshoe Kidney With Hydronephrosis - Tales of The UnexpectedDocument3 pages(03241750 - Acta Medica Bulgarica) Horseshoe Kidney With Hydronephrosis - Tales of The UnexpectedTeodorNo ratings yet
- Hartley Final PDFDocument16 pagesHartley Final PDFAlexandriaJoNo ratings yet
- Introduction Urinary SystemDocument19 pagesIntroduction Urinary SystemKatherine Anne ReyesNo ratings yet
- Biliary Surgery: Presenter: DR Muhuga JR Facilitator: DR MwashambwaDocument54 pagesBiliary Surgery: Presenter: DR Muhuga JR Facilitator: DR MwashambwaSamar AhmadNo ratings yet
- V63N1A08Document7 pagesV63N1A08Carolina JozamiNo ratings yet
- Ga Kebaca (Blabla)Document5 pagesGa Kebaca (Blabla)Fika Khulma SofiaNo ratings yet
- Upjo Surgical ManagementDocument54 pagesUpjo Surgical ManagementUsmle GuyNo ratings yet
- Colorectal Surgery: Clinical Care and ManagementFrom EverandColorectal Surgery: Clinical Care and ManagementBruce GeorgeNo ratings yet
- Jo No Entry Site 05202016Document38 pagesJo No Entry Site 05202016sirrfsNo ratings yet
- Dance - Davis Intubated Ureterotomy in A Child - 05202016Document27 pagesDance - Davis Intubated Ureterotomy in A Child - 05202016sirrfsNo ratings yet
- Embedded Inferior Vena Cava Filter RemovalDocument20 pagesEmbedded Inferior Vena Cava Filter RemovalsirrfsNo ratings yet
- Large Nonmalignant Hepatic Mass and Role of Pediatric Interventional RadiologyDocument26 pagesLarge Nonmalignant Hepatic Mass and Role of Pediatric Interventional RadiologysirrfsNo ratings yet
- ICU Clinical GoalsDocument4 pagesICU Clinical GoalssirrfsNo ratings yet
- Pediatric Partial Splenic EmbolizationDocument8 pagesPediatric Partial Splenic EmbolizationsirrfsNo ratings yet
- Vascular Surgery Rotation Clinical Goals For I R TraineesDocument5 pagesVascular Surgery Rotation Clinical Goals For I R TraineessirrfsNo ratings yet
- Not Simply A Fibroid Uterus: A Rare Diagnostic DiscoveryDocument17 pagesNot Simply A Fibroid Uterus: A Rare Diagnostic DiscoverysirrfsNo ratings yet
- Jo Boy With SOB 04202016Document25 pagesJo Boy With SOB 04202016sirrfsNo ratings yet
- Zachary Liner SplenicVeinRecanalization 04102016Document31 pagesZachary Liner SplenicVeinRecanalization 04102016sirrfsNo ratings yet
- Bahl - Embolization of A Type II Endoleak Using Onyx - 02012016Document22 pagesBahl - Embolization of A Type II Endoleak Using Onyx - 02012016sirrfsNo ratings yet
- Raff Recurrent Pyogenic Cholangitis 03012016Document30 pagesRaff Recurrent Pyogenic Cholangitis 03012016sirrfsNo ratings yet
- Lamparello CVOcclusion 02102016Document16 pagesLamparello CVOcclusion 02102016sirrfsNo ratings yet
- Pediatric G Tube Placement ComplicationsDocument8 pagesPediatric G Tube Placement ComplicationssirrfsNo ratings yet
- Landmark Vs Ultrasound CVA Journal PrimerDocument8 pagesLandmark Vs Ultrasound CVA Journal PrimersirrfsNo ratings yet
- Paracentesis - SIR GGR Survival GuideDocument4 pagesParacentesis - SIR GGR Survival GuidesirrfsNo ratings yet
- Fundamentals of Pediatric Central Venous AccessDocument38 pagesFundamentals of Pediatric Central Venous AccesssirrfsNo ratings yet
- Lim The Great Houdini 02012016Document19 pagesLim The Great Houdini 02012016sirrfsNo ratings yet
- Angioplasty For RAS Journal PrimerDocument8 pagesAngioplasty For RAS Journal PrimersirrfsNo ratings yet
- Vyas RUQAneurysm 01202016Document18 pagesVyas RUQAneurysm 01202016sirrfs100% (1)
- Evans - Unusual Presentation of Superior Vena Cava Syndrome - 12012015Document17 pagesEvans - Unusual Presentation of Superior Vena Cava Syndrome - 12012015sirrfsNo ratings yet
- Natour IVCFILTERthrombosis 01102016Document35 pagesNatour IVCFILTERthrombosis 01102016sirrfsNo ratings yet
- Vyas Brto 12202015Document21 pagesVyas Brto 12202015sirrfsNo ratings yet
- Vertebroplasty and Kyphoplasty Neuro JPDocument8 pagesVertebroplasty and Kyphoplasty Neuro JPsirrfsNo ratings yet
- Lumbar ESI - SIR Pain Survival GuideDocument4 pagesLumbar ESI - SIR Pain Survival GuidesirrfsNo ratings yet
- PEITHO Trial: Fibrinolysis For Patients With IntermediateDocument9 pagesPEITHO Trial: Fibrinolysis For Patients With IntermediatesirrfsNo ratings yet
- Spinal Facet Injection-SIR Pain Survival GuideDocument3 pagesSpinal Facet Injection-SIR Pain Survival GuidesirrfsNo ratings yet
- ODell Lipsarcoma 12102015Document24 pagesODell Lipsarcoma 12102015sirrfs100% (1)
- Gastrosotomy RadiationDocument9 pagesGastrosotomy RadiationsirrfsNo ratings yet
- Surgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Document7 pagesSurgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Ayu DinaNo ratings yet
- DPP 2 Oesophagus and StomachDocument4 pagesDPP 2 Oesophagus and StomachDr-Atin Kumar SrivastavaNo ratings yet
- Acute Infectious DiarrheaDocument3 pagesAcute Infectious DiarrheaHera Yayang LoidsNo ratings yet
- Science 6 - 2nd Quarterly Exam (Grade 6)Document4 pagesScience 6 - 2nd Quarterly Exam (Grade 6)Brian BuiserNo ratings yet
- PANCREATITIS: CAUSES, SIGNS, SYMPTOMS AND NURSING MANAGEMENTDocument23 pagesPANCREATITIS: CAUSES, SIGNS, SYMPTOMS AND NURSING MANAGEMENTYasir Mumtaz100% (1)
- 1.study of Physiological Functions of Digestive System of Farm AnimalsDocument58 pages1.study of Physiological Functions of Digestive System of Farm AnimalsKashifNo ratings yet
- Organs of The Digestive System and Their FunctionsDocument2 pagesOrgans of The Digestive System and Their FunctionsChari Mae Tamayo Panganiban100% (1)
- Liver - Dr. Allam 2021 PDFDocument70 pagesLiver - Dr. Allam 2021 PDFMohammedNo ratings yet
- Histo Lab Ex 13 17Document57 pagesHisto Lab Ex 13 17Allyzha AguilarNo ratings yet
- Pancreatic and Duodenal Injuries UpdateDocument59 pagesPancreatic and Duodenal Injuries UpdateAndrie KundrieNo ratings yet
- Chronic Transaminitis 07Document39 pagesChronic Transaminitis 07Jessica GarletsNo ratings yet
- Chapter 5 and 6 Nutrition in Humans (CE - Structured Questions Marking Scheme)Document5 pagesChapter 5 and 6 Nutrition in Humans (CE - Structured Questions Marking Scheme)Emily LiNo ratings yet
- Pi Is 2468448120302800Document2 pagesPi Is 2468448120302800Shivaraj S ANo ratings yet
- Anaphy Reviiewer - RabeDocument16 pagesAnaphy Reviiewer - RabeAyessa Marie BarbosaNo ratings yet
- Abdomen and Gastrointestin Al (Git) Imaging: Prof. Qurashi M. AliDocument47 pagesAbdomen and Gastrointestin Al (Git) Imaging: Prof. Qurashi M. AliIbrahim BabikirNo ratings yet
- Pizza Digestion High School ReportDocument4 pagesPizza Digestion High School ReportBrad KNo ratings yet
- Gross Anatomy & Histology of Liver: Prepared By: Anish Dhakal (Aryan) MBBS Student Patan Academy of Health SciencesDocument21 pagesGross Anatomy & Histology of Liver: Prepared By: Anish Dhakal (Aryan) MBBS Student Patan Academy of Health SciencesAjeng TunjungputriNo ratings yet
- JAUNDICE-Early Clinical ExposureDocument42 pagesJAUNDICE-Early Clinical Exposurevarshita5905No ratings yet
- Neonatal Intestinal Obstructions: Causes, Symptoms and TreatmentsDocument21 pagesNeonatal Intestinal Obstructions: Causes, Symptoms and Treatmentsdtalks andyouNo ratings yet
- Quiz GITDocument3 pagesQuiz GITSuzana YusofNo ratings yet
- Gallbladder Surgery: Common FAQ & Myths - Kaizen Gastro CareDocument2 pagesGallbladder Surgery: Common FAQ & Myths - Kaizen Gastro CareKaizen Gastro CareNo ratings yet
- Acute Cholecystitis & Gallbladder Polyp Imaging FindingsDocument30 pagesAcute Cholecystitis & Gallbladder Polyp Imaging FindingsCaitlin Joy Cardel MendozaNo ratings yet
- GERD2Document28 pagesGERD2Anonymous 2qUGvwI9No ratings yet
- Digestive Domain GuideDocument31 pagesDigestive Domain Guidemina000005No ratings yet
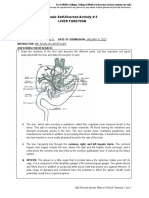
- Finals Self-Directed Activity # 3 Liver FunctionDocument7 pagesFinals Self-Directed Activity # 3 Liver FunctionAIRA GIN G. ARELLANONo ratings yet
- IHD stone treatmentDocument49 pagesIHD stone treatmentFitriardi SejatiNo ratings yet
- Chapter 8 - Digestive SystemDocument96 pagesChapter 8 - Digestive Systemfit3akmal0% (1)
- Colostomy CareDocument49 pagesColostomy Caregladz25100% (1)
- Chapter 6 Nutrition in HumansDocument3 pagesChapter 6 Nutrition in Humansno one0% (1)
- Lab1 - Digestion Rate On FishDocument9 pagesLab1 - Digestion Rate On FishAdeniaNo ratings yet