You might also like
- EKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture SeriesDocument85 pagesEKG Interpretation: UNS Cardiovascular Dept Medical Student Lecture Seriesandina rosmalianti100% (1)
- TH4-127 KreuzDocument113 pagesTH4-127 Kreuzakp892818No ratings yet
- Interpretasi ElektrokardiografiDocument60 pagesInterpretasi ElektrokardiografiAditya Praja'schNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesWidya Surya AvantiNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDyah Ajeng PratiwiNo ratings yet
- Interpretasi ElektrokardiogramDocument36 pagesInterpretasi ElektrokardiogramendahNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesRenn Karlo LindoNo ratings yet
- ECG Lecture 4Document44 pagesECG Lecture 4asdasdasdasNo ratings yet
- Ecg enDocument12 pagesEcg enKeep smileNo ratings yet
- ECG InterpretationDocument168 pagesECG InterpretationPavi YaskarthiNo ratings yet
- Ekg Panum or OsceDocument69 pagesEkg Panum or OsceGladish RindraNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesHasnahdurrNo ratings yet
- EKG InterpretationDocument58 pagesEKG InterpretationHasnahdurrNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesanisaNo ratings yet
- Ekg by DR RezaDocument105 pagesEkg by DR RezaYoga KarsendaNo ratings yet
- EKG InterpretationDocument58 pagesEKG InterpretationIman Sama-aliNo ratings yet
- ECG ExaminationDocument70 pagesECG ExaminationPercy Caceres OlivaresNo ratings yet
- Interpretasi Elektrokardiografi: Dr. Erlina Marfianti, MSC, SPPD Departemen Ilmu Penyakit Dalam Fakultas Kedokteran UiiDocument60 pagesInterpretasi Elektrokardiografi: Dr. Erlina Marfianti, MSC, SPPD Departemen Ilmu Penyakit Dalam Fakultas Kedokteran UiiArif Zulfian MubarokNo ratings yet
- Interpretasi ElektrokardiografiDocument60 pagesInterpretasi ElektrokardiografiYogi GustriansyahNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesNathalia ValdesNo ratings yet
- EKG Interpretation: DR K P Tripathy Kims, BhubaneswarDocument58 pagesEKG Interpretation: DR K P Tripathy Kims, BhubaneswarAbhilash MohantyNo ratings yet
- EKG Interpretation 1Document56 pagesEKG Interpretation 1usmleusmle86No ratings yet
- Electrocardiograms (Ecgs)Document80 pagesElectrocardiograms (Ecgs)heena solankiNo ratings yet
- Rudiments of ECGDocument101 pagesRudiments of ECGJacekNo ratings yet
- ECG Reading: The Common and DangerousDocument77 pagesECG Reading: The Common and DangerousFitri UlansariNo ratings yet
- ECGDocument33 pagesECGTamia PutriNo ratings yet
- INTERPRETASI EKG MahasiswaDocument43 pagesINTERPRETASI EKG MahasiswaMartin Susanto, MDNo ratings yet
- Basic Ecg: - Department of Medicine BIMC Hospital 2013Document60 pagesBasic Ecg: - Department of Medicine BIMC Hospital 2013LexadkNo ratings yet
- EKG - Interpretation FK UNRIDocument51 pagesEKG - Interpretation FK UNRIYenni LisnawatiNo ratings yet
- 5 Ekg PM Eng PDFDocument70 pages5 Ekg PM Eng PDFfgxNo ratings yet
- Ecg Abnormal 1-HpwDocument77 pagesEcg Abnormal 1-HpwAndre JuliantNo ratings yet
- ECG Brief NotesDocument5 pagesECG Brief NotesKalpani Malsha UdawelagedaraNo ratings yet
- ECG Demographics Rate: 300/# Large Box in RR IntervalDocument11 pagesECG Demographics Rate: 300/# Large Box in RR IntervalJonathan DavisNo ratings yet
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- Approach To Ecgs: Rhythm Check RateDocument5 pagesApproach To Ecgs: Rhythm Check RateAnanda NadaradjaneNo ratings yet
- A Simplified ECG GuideDocument4 pagesA Simplified ECG GuidecherryNo ratings yet
- ECG Kursus FKUSU DR A.majid 05 Juni 2007Document37 pagesECG Kursus FKUSU DR A.majid 05 Juni 2007Shinta LissevaNo ratings yet
- The Normal Adult ECGDocument84 pagesThe Normal Adult ECGkimiastroNo ratings yet
- EKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesDocument58 pagesEKG Interpretation: UNC Emergency Medicine Medical Student Lecture SeriesrsadellaNo ratings yet
- ECG Master Class-3Document97 pagesECG Master Class-3Shohag ID CenterNo ratings yet
- Interpretasi ECG Dr. SallyDocument66 pagesInterpretasi ECG Dr. SallyRichard GunawanNo ratings yet
- ELECTROCARDIOGRAPHYDocument75 pagesELECTROCARDIOGRAPHYMeliaNo ratings yet
- Hotel Dpalma, Bandung 16 Maret 2018: Dr. Benny Prasetya PDocument145 pagesHotel Dpalma, Bandung 16 Maret 2018: Dr. Benny Prasetya PkangheriNo ratings yet
- ECG SummaryDocument11 pagesECG Summaryjackfruit5887No ratings yet
- Dr. Adeel Ahmed Waheed: House Officer M-4Document84 pagesDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNo ratings yet
- Matrikulasi Interpretasi EkgDocument40 pagesMatrikulasi Interpretasi Ekgsupergirl2123No ratings yet
- Ekg MorphologyDocument1 pageEkg MorphologyTeresa MartinsNo ratings yet
- 16.1. ECG 3 (Arryhtmia) -肖培林Document77 pages16.1. ECG 3 (Arryhtmia) -肖培林mirabel IvanaliNo ratings yet
- Basics of Ecg: DR Shyama Assistant Professor General Medicine Aiims, PatnaDocument117 pagesBasics of Ecg: DR Shyama Assistant Professor General Medicine Aiims, PatnaSimran KothariNo ratings yet
- TH TH TH THDocument9 pagesTH TH TH THAlex PengNo ratings yet
- ECG InterpretationDocument83 pagesECG InterpretationJuana Maria Garcia Espinoza100% (2)
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (9)
- Ecg Presentation 2013Document40 pagesEcg Presentation 2013Samuel FpNo ratings yet
- Electrocardiograms (Ecgs)Document86 pagesElectrocardiograms (Ecgs)nana wandhanaNo ratings yet
- 5 ECG Interpretation With AnswersDocument48 pages5 ECG Interpretation With AnswersQusai Ibraheem100% (1)
- Cheong Kuan Loong Medical Department Hospital Sultan Haji Ahmad Shah, Temerloh 12/5/10Document99 pagesCheong Kuan Loong Medical Department Hospital Sultan Haji Ahmad Shah, Temerloh 12/5/10Haq10No ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- Epidural and Non-Epidural Analgesia in LabourDocument127 pagesEpidural and Non-Epidural Analgesia in Labourskycall28No ratings yet
- Collagen ShieldDocument24 pagesCollagen ShieldDina WahyuNo ratings yet
- Guidelines For Vaccination in Normal Adults in IndiaDocument12 pagesGuidelines For Vaccination in Normal Adults in Indiaskycall28No ratings yet
- Sub Centers in Indian HealthcareDocument80 pagesSub Centers in Indian Healthcareskycall28No ratings yet
- Seminar: Course Instructor-Prof Dr. S. DharaDocument14 pagesSeminar: Course Instructor-Prof Dr. S. Dharaskycall28No ratings yet
- Biodegradable Polymers As BiomaterialsDocument37 pagesBiodegradable Polymers As BiomaterialsNguyen LucNo ratings yet
- Brain Tumour Extraction From MRI Images Using MATLABDocument4 pagesBrain Tumour Extraction From MRI Images Using MATLABKoshy Geoji0% (1)
- Mri Gradients Phase and Frequency EncodingDocument25 pagesMri Gradients Phase and Frequency Encodingskycall28No ratings yet
- BuildingaMedVocabulary PDFDocument10 pagesBuildingaMedVocabulary PDFTimnemNo ratings yet
- 7b821ce7bf9920b2c3dbe5d1ce526c93Document2 pages7b821ce7bf9920b2c3dbe5d1ce526c93laptopsftwNo ratings yet
- 7b821ce7bf9920b2c3dbe5d1ce526c93Document2 pages7b821ce7bf9920b2c3dbe5d1ce526c93laptopsftwNo ratings yet
- Basic Concepts of CNS FunctionsDocument25 pagesBasic Concepts of CNS Functionsskycall28No ratings yet
- UltraSound LectureDocument32 pagesUltraSound Lectureskycall28No ratings yet
- Part Pinouts: "Think of An Op-Amp As For Feedback." - Horowitz and HillDocument1 pagePart Pinouts: "Think of An Op-Amp As For Feedback." - Horowitz and Hillskycall28No ratings yet
- Radiology, Radiotherapy Notes To PGDocument16 pagesRadiology, Radiotherapy Notes To PGskycall28No ratings yet
- How Do You Know When You Have A Stress FractureDocument5 pagesHow Do You Know When You Have A Stress Fractureskycall28No ratings yet
- Zika Virus and Birth DefectsDocument7 pagesZika Virus and Birth Defectsskycall28No ratings yet
- Quantum Mechanics Practice Test PDFDocument7 pagesQuantum Mechanics Practice Test PDFskycall28No ratings yet
- BiodieselDocument14 pagesBiodieselskycall28No ratings yet
- Math Better Explained (Exponentials and E)Document11 pagesMath Better Explained (Exponentials and E)skycall28No ratings yet
- 44-Incidence, 45 Notes To PG PDFDocument5 pages44-Incidence, 45 Notes To PG PDFskycall28No ratings yet
- Krita 2.9 Layer StackDocument4 pagesKrita 2.9 Layer Stackskycall28No ratings yet
- Introducing The Blind Man Technique-Study Less and Retain MoreDocument9 pagesIntroducing The Blind Man Technique-Study Less and Retain Moreskycall28No ratings yet
- HUD For XubuntuDocument6 pagesHUD For Xubuntuskycall28No ratings yet
- 45 Notes To PG: 45-ExceptionsDocument8 pages45 Notes To PG: 45-ExceptionsNikhil KanikaNo ratings yet
- The Many Uses of GcalDocument9 pagesThe Many Uses of Gcalskycall28No ratings yet
- Skin Notes For PGDocument11 pagesSkin Notes For PGskycall28No ratings yet
- Cell, Body and Stain NotesDocument7 pagesCell, Body and Stain Notesskycall28No ratings yet
- Legal Procedures Notes For PGDocument7 pagesLegal Procedures Notes For PGskycall28No ratings yet
- Scale, Score, Criteria, Grading, Index NotesDocument13 pagesScale, Score, Criteria, Grading, Index Notesskycall28No ratings yet
- 9515-184-51-ENG - REV - B1 HScribe Clinicians Guide V5 - 01Document48 pages9515-184-51-ENG - REV - B1 HScribe Clinicians Guide V5 - 01Rodrigo GutierrezNo ratings yet
- Lesson 2 Adult Resuscitation v3 1Document16 pagesLesson 2 Adult Resuscitation v3 1Michels Garments S.H Nawaz HosieryNo ratings yet
- Level of Fibrinogen and Risk of Fatal and Non-Fatal Stroke. EUROSTROKE: A Collaborative Study Among Research Centres in EuropeDocument5 pagesLevel of Fibrinogen and Risk of Fatal and Non-Fatal Stroke. EUROSTROKE: A Collaborative Study Among Research Centres in EuropeThein Htun NaungNo ratings yet
- Cardiovascular Examination 1Document43 pagesCardiovascular Examination 1ערין גבאריןNo ratings yet
- Mrcp-PACES 2023 - Sequence - CVSDocument2 pagesMrcp-PACES 2023 - Sequence - CVSvaranasidineshNo ratings yet
- DapusDocument2 pagesDapusAdhi CandraNo ratings yet
- Pearls of MRCP Part 2 PastestDocument111 pagesPearls of MRCP Part 2 PastestS TNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612YassarNo ratings yet
- All Past Rounds Cardio MCQs AlexandriaDocument37 pagesAll Past Rounds Cardio MCQs AlexandriaMahmoud Abouelsoud100% (1)
- Acc Ecg ChallengeDocument91 pagesAcc Ecg ChallengeMiguel LizarragaNo ratings yet
- Mitral StenosisDocument17 pagesMitral StenosisMuhammad Alauddin Sarwar100% (8)
- Case Report - Rifkia Izza Maorits & Risfandi Ahmad TaskuraDocument8 pagesCase Report - Rifkia Izza Maorits & Risfandi Ahmad TaskuraAnonymous aTPgWhNo ratings yet
- Chronic Heart Failure Case FileDocument2 pagesChronic Heart Failure Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosis Pathophysiolog Y Planning Intervention Rationale EvaluationDocument1 pageNovilyn C. Pataray BSN - Ii: Assessment Diagnosis Pathophysiolog Y Planning Intervention Rationale EvaluationCharina Aubrey100% (3)
- Unleash Benefit of Metoprolol in CCS Applying Evidence Into PracticeDocument35 pagesUnleash Benefit of Metoprolol in CCS Applying Evidence Into PracticeEdelweisscynaNo ratings yet
- 7.vital SignDocument44 pages7.vital SignRobiatulAdawiyahNo ratings yet
- Cardiopulmonary Resuscitation Update: Continuing Education ColumnDocument9 pagesCardiopulmonary Resuscitation Update: Continuing Education Columnkang soon cheolNo ratings yet
- Point-Of-Care Ultrasound in Cardiac ArrestDocument13 pagesPoint-Of-Care Ultrasound in Cardiac ArrestEgorSazhaevNo ratings yet
- XXX. MCQ Cardiovascular System Book 315-336Document19 pagesXXX. MCQ Cardiovascular System Book 315-336Maria OnofreiNo ratings yet
- Antianginal and Antiischemic DrugsDocument18 pagesAntianginal and Antiischemic DrugsNaveen KumarNo ratings yet
- Nursing Care Plan For Coronary Artery DiseaseDocument3 pagesNursing Care Plan For Coronary Artery DiseaseLorraineAnneSantiagoCandelario91% (22)
- Handouts - Cardio - Dr. Arreglo (Nov 2023)Document92 pagesHandouts - Cardio - Dr. Arreglo (Nov 2023)Paola Jane OrioNo ratings yet
- Assessment of Breathlessness Clinical Pathway Assessment HandoutDocument8 pagesAssessment of Breathlessness Clinical Pathway Assessment HandoutShivaniNo ratings yet
- Materi VHD - DR - Achmad PutraDocument44 pagesMateri VHD - DR - Achmad PutraDila AswitaliaNo ratings yet
- Atrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhDocument60 pagesAtrial Septal Defect: Presented By:-Dr Kunwar Sidharth SaurabhKunwar Sidharth SaurabhNo ratings yet
- Management of Hypertension: Affan Syafiqi - Nurul Husna - Audi RahmanDocument77 pagesManagement of Hypertension: Affan Syafiqi - Nurul Husna - Audi RahmanRavi K. ShuklaNo ratings yet
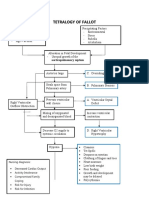
- Concept Map Tetralogy of FallotDocument2 pagesConcept Map Tetralogy of FallotKarl KiwisNo ratings yet
- KMR ACLS Helpful Hints 2015 Guidelines Version 1 0 Revised 1 PDFDocument2 pagesKMR ACLS Helpful Hints 2015 Guidelines Version 1 0 Revised 1 PDFSheenaMilesNo ratings yet
- Atrial Septal DefectDocument2 pagesAtrial Septal DefectElizabethNo ratings yet
- Cardio OoooDocument11 pagesCardio OoooBrian BaggayanNo ratings yet