You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 52 Ioc Scientific ScheduleDocument15 pages52 Ioc Scientific ScheduleCM Panda CedeesNo ratings yet
- 22nd Ios PG Students ConventionDocument2 pages22nd Ios PG Students ConventionCM Panda CedeesNo ratings yet
- Cytotoxit of AlginatsDocument6 pagesCytotoxit of AlginatsCM Panda CedeesNo ratings yet
- Craniofacial GrowthDocument21 pagesCraniofacial GrowthAnu YaraganiNo ratings yet
- Ceph HandoutDocument18 pagesCeph Handoutwaheguru13he13No ratings yet
- 0 FCFD 5058 F 9 e 4 Adff 7000000Document9 pages0 FCFD 5058 F 9 e 4 Adff 7000000CM Panda CedeesNo ratings yet
- Cozzani2013 MIXED DENTITIONDocument7 pagesCozzani2013 MIXED DENTITIONCM Panda Cedees100% (1)
- Evolution Epidemiology and Etiology of Temporomandibular Joint DisordersDocument6 pagesEvolution Epidemiology and Etiology of Temporomandibular Joint DisordersCM Panda CedeesNo ratings yet
- Revised Vacancy Position of July 201624may2016143027Document1 pageRevised Vacancy Position of July 201624may2016143027CM Panda CedeesNo ratings yet
- Lad Eira 2012Document10 pagesLad Eira 2012CM Panda CedeesNo ratings yet
- Houghton1977 002Document5 pagesHoughton1977 002CM Panda CedeesNo ratings yet
- Se PeratorsDocument6 pagesSe PeratorsCM Panda CedeesNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SS 102 S5 - Final ExamDocument3 pagesSS 102 S5 - Final ExamTabish HamidNo ratings yet
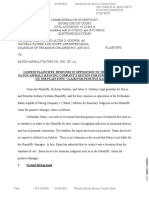
- Johnson Claims Against Eaton AsphaltDocument39 pagesJohnson Claims Against Eaton AsphaltCincinnatiEnquirerNo ratings yet
- Chraj 1Document6 pagesChraj 1The Independent GhanaNo ratings yet
- I.I.M.U.N. Coimbatore Kids Module 2021Document7 pagesI.I.M.U.N. Coimbatore Kids Module 2021Midhun Bhuvanesh.B 7ANo ratings yet
- Destination Visalia, CA - 2011 / 2012 1Document44 pagesDestination Visalia, CA - 2011 / 2012 1DowntownVisaliaNo ratings yet
- KWPL07 RankinDocument28 pagesKWPL07 RankinBoogy GrimNo ratings yet
- Image Saving, Processing and Name Tagging Over SDTP Using Java ScriptDocument21 pagesImage Saving, Processing and Name Tagging Over SDTP Using Java Scriptsomnath banerjeeNo ratings yet
- Lesson 2 - Pure Substances and MixturesDocument41 pagesLesson 2 - Pure Substances and Mixturescecil tayagNo ratings yet
- Wed 0945-Avionics Modernization For LegacyDocument38 pagesWed 0945-Avionics Modernization For LegacygasparferrerNo ratings yet
- Krok 1 Stomatology: Test Items For Licensing ExaminationDocument28 pagesKrok 1 Stomatology: Test Items For Licensing ExaminationhelloNo ratings yet
- SUMMATIVE Entrep Q1Document2 pagesSUMMATIVE Entrep Q1ocsapwaketsNo ratings yet
- Life After Life by Kate AtkinsonDocument25 pagesLife After Life by Kate AtkinsonRandom House of Canada60% (15)
- How To Argue A CaseDocument5 pagesHow To Argue A CaseItam HillNo ratings yet
- Dauns Prime Module 1978Document26 pagesDauns Prime Module 1978Ivan AdrianNo ratings yet
- Map of Jeju: For Muslim TouristsDocument7 pagesMap of Jeju: For Muslim TouristslukmannyeoNo ratings yet
- Quality TranslationDocument33 pagesQuality TranslationCarolina ContrerasNo ratings yet
- Teaching The GospelDocument50 pagesTeaching The GospelgabrielpoulsonNo ratings yet
- Former UM Soccer Coach Sues University For DefamationDocument12 pagesFormer UM Soccer Coach Sues University For DefamationNBC MontanaNo ratings yet
- Set 1 Questions 1-20Document10 pagesSet 1 Questions 1-20aeda80No ratings yet
- Narrations - Direct and Indirect SpeehesDocument6 pagesNarrations - Direct and Indirect Speehesskitteringkite100% (1)
- A Multivariate Model For Analyzing Crime Scene InformationDocument26 pagesA Multivariate Model For Analyzing Crime Scene InformationNorberth Ioan OkrosNo ratings yet
- California Law of Perscriptive EasementsDocument3 pagesCalifornia Law of Perscriptive EasementsSylvester MooreNo ratings yet
- Statement by The Ukrainian Canadian CongressDocument1 pageStatement by The Ukrainian Canadian CongressLevon SevuntsNo ratings yet
- Contoh MOTIVATION LETTERDocument19 pagesContoh MOTIVATION LETTERDavin Tiska AbrianiNo ratings yet
- Airworthiness Directive: Design Approval Holder's Name: Type/Model Designation(s)Document4 pagesAirworthiness Directive: Design Approval Holder's Name: Type/Model Designation(s)Kris Wuthrich BatarioNo ratings yet
- XXXXXDocument38 pagesXXXXXGarrett HughesNo ratings yet
- Risk Management NotesDocument27 pagesRisk Management NoteskomalNo ratings yet
- Lesson 4 Prepare and Interpret Technical Drawing: Alphabet of LinesDocument26 pagesLesson 4 Prepare and Interpret Technical Drawing: Alphabet of LinesREYNALDO BAJADONo ratings yet
- Family Law Outline RevisedDocument11 pagesFamily Law Outline RevisedAdriana CarinanNo ratings yet
- 1 Partnership FormationDocument7 pages1 Partnership FormationJ MahinayNo ratings yet