You might also like
- Pulpal Access Cavities & ErrorsDocument20 pagesPulpal Access Cavities & ErrorsLinh PhanNo ratings yet
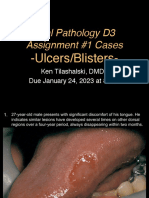
- D3 Ulcers Blisters Cases Due01242023 8amDocument13 pagesD3 Ulcers Blisters Cases Due01242023 8amLinh PhanNo ratings yet
- 1 Histology of The Small and Large IntestineDocument9 pages1 Histology of The Small and Large IntestineLinh PhanNo ratings yet
- Endodontic Case Complexity and Working With The Specialist No VoiceDocument14 pagesEndodontic Case Complexity and Working With The Specialist No VoiceLinh PhanNo ratings yet
- 5 Intestinal Fluid and Electrolyte Transport-1Document9 pages5 Intestinal Fluid and Electrolyte Transport-1Linh PhanNo ratings yet
- 3 Gi Motility (Parts I-Iv) Swallowing & Esophageal MotilityDocument11 pages3 Gi Motility (Parts I-Iv) Swallowing & Esophageal MotilityLinh PhanNo ratings yet
- 2 Histology of The Liver, Gallbladder, and Pancreas - 2Document11 pages2 Histology of The Liver, Gallbladder, and Pancreas - 2Linh PhanNo ratings yet
- 4 Gastrointestinal Physiology - Digestion and AbsorptionDocument11 pages4 Gastrointestinal Physiology - Digestion and AbsorptionLinh PhanNo ratings yet
- 2 Anatomy of The Abdominal VisceraDocument9 pages2 Anatomy of The Abdominal VisceraLinh PhanNo ratings yet
- 3 Pancreatic and Biliary SecretionDocument11 pages3 Pancreatic and Biliary SecretionLinh PhanNo ratings yet
- 1 Introduction To The Gastrointestinal SystemDocument7 pages1 Introduction To The Gastrointestinal SystemLinh Phan100% (1)
- 4 GI Hormones I: Endocrine HormonesDocument4 pages4 GI Hormones I: Endocrine HormonesLinh PhanNo ratings yet
- 5 Gi Hormones Ii: Paracrine HormonesDocument2 pages5 Gi Hormones Ii: Paracrine HormonesLinh PhanNo ratings yet
- Chemical ElementDocument2 pagesChemical ElementLinh PhanNo ratings yet
- AnestesiDocument16 pagesAnestesifarissa utamiNo ratings yet
- 7 Histology of The Oral Cavity and Salivary GlandsDocument11 pages7 Histology of The Oral Cavity and Salivary GlandsLinh PhanNo ratings yet
- CrystallizationDocument4 pagesCrystallizationLinh PhanNo ratings yet
- Biomaterials 2005 26 2603 Yang Et Al Electrospun Neuro EngDocument8 pagesBiomaterials 2005 26 2603 Yang Et Al Electrospun Neuro EngLinh PhanNo ratings yet
- L2 Electromagnetic RadiationDocument15 pagesL2 Electromagnetic RadiationLinh PhanNo ratings yet
- PPT1 Chap 4 Zhang StudentDocument103 pagesPPT1 Chap 4 Zhang StudentLinh PhanNo ratings yet
- Pre-Lab Quiz I (238) - SP2017 CH 238-Q8 Organic Chemistry II LabDocument8 pagesPre-Lab Quiz I (238) - SP2017 CH 238-Q8 Organic Chemistry II LabLinh PhanNo ratings yet
- Recomandation LetterDocument2 pagesRecomandation LetterLinh PhanNo ratings yet
- L14 UltrasoundDocument27 pagesL14 UltrasoundLinh PhanNo ratings yet
- Biomechanics Design Lab Presentation FINALDocument27 pagesBiomechanics Design Lab Presentation FINALLinh PhanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Manual de Partes Ricoh MPC2050 PDFDocument314 pagesManual de Partes Ricoh MPC2050 PDFLuis AlbertoNo ratings yet
- The Distinctive Musical Styles and Characteristics of Expressionism in Music Through The Elements of MusicDocument4 pagesThe Distinctive Musical Styles and Characteristics of Expressionism in Music Through The Elements of MusicRoan BodinoNo ratings yet
- Disney Luxury Homes in Hyderabad's Financial DistrictDocument21 pagesDisney Luxury Homes in Hyderabad's Financial DistrictKota RavichandNo ratings yet
- 02TP PrelimExam MITDocument2 pages02TP PrelimExam MITSnapShop by AJNo ratings yet
- Sherlock Holmes and The Strange MR Angel TEXTDocument15 pagesSherlock Holmes and The Strange MR Angel TEXTPaulo ShimidtNo ratings yet
- Gillian Golosky ResumeDocument2 pagesGillian Golosky Resumeapi-435351626No ratings yet
- Dance in Ancient EgyptDocument12 pagesDance in Ancient EgyptMohamed Abd El LatefNo ratings yet
- Gymnastics Module2 1stsemDocument23 pagesGymnastics Module2 1stsemJhon Cleoh DiasaNo ratings yet
- Dennis BurtonDocument1 pageDennis Burtonapoorva_mandavilliNo ratings yet
- Golf Ball DiverDocument8 pagesGolf Ball DiverDaik NarevachNo ratings yet
- Easy Chinese Recipes PDFDocument151 pagesEasy Chinese Recipes PDFTrafalgar100% (10)
- Walkthrough - Sheet 0.50Document12 pagesWalkthrough - Sheet 0.50mysexylove50No ratings yet
- SBB - Online Timetable - lsn-GVADocument2 pagesSBB - Online Timetable - lsn-GVAlbo33No ratings yet
- Galilee Division Youth Fellowship and Leaders AnnouncedDocument5 pagesGalilee Division Youth Fellowship and Leaders AnnouncedJohn Carlo EstoyNo ratings yet
- Comparatives and Superlatives of AdjectivesDocument5 pagesComparatives and Superlatives of AdjectivesTố UyênNo ratings yet
- Kasut You 2.3Document21 pagesKasut You 2.3AdamZain788No ratings yet
- 1 48Document48 pages1 48rdvreyNo ratings yet
- Advanced Buttercream Recipes - Tasty and Intricate Buttercream Recipes For Gourmet Cakes and CupcakesDocument64 pagesAdvanced Buttercream Recipes - Tasty and Intricate Buttercream Recipes For Gourmet Cakes and CupcakesAllen NorthNo ratings yet
- RotationDocument4 pagesRotationapi-431813813No ratings yet
- Thieves' World Murder at The Vulgar Unicorn (d20)Document81 pagesThieves' World Murder at The Vulgar Unicorn (d20)Red Stone100% (4)
- The Second Emerging Expression Biennial: The Artist and The ComputerDocument4 pagesThe Second Emerging Expression Biennial: The Artist and The Computerdonkey slapNo ratings yet
- Toshiba Laptop Netbook Pricelist - September 2010Document8 pagesToshiba Laptop Netbook Pricelist - September 2010Praveen G. MenonNo ratings yet
- Daemornia - Core RulebookDocument219 pagesDaemornia - Core RulebookVEX - HAN - 092No ratings yet
- Mr Otis and the Canterville GhostDocument3 pagesMr Otis and the Canterville GhostPatricia Pérez BerradeNo ratings yet
- Art of Film Syllabus PDFDocument9 pagesArt of Film Syllabus PDFKevin100% (1)
- Reviewer Pe12Document5 pagesReviewer Pe12PoyporoypoyNo ratings yet
- MFL69365752 01 PDFDocument292 pagesMFL69365752 01 PDFGeorgescu FlorentinNo ratings yet
- Abb Switch Disconnectors 1Document3 pagesAbb Switch Disconnectors 1Farid GergesNo ratings yet
- Cultural Diversity and Influences Shaped Indonesian MusicDocument12 pagesCultural Diversity and Influences Shaped Indonesian MusicjhokenNo ratings yet
- International Student Guide to Study and Work PermitsDocument7 pagesInternational Student Guide to Study and Work PermitsBlazing FastNo ratings yet