You might also like
- Social Skills WorksheetsDocument26 pagesSocial Skills WorksheetsHusaini100% (5)
- Musculoskeletal NotesDocument4 pagesMusculoskeletal NotesFreeNursingNotes100% (1)
- NP Outreach Curriculum in Rheumatology St. Joseph's Health Care, London, ON Dr. Sherry Rohekar November 12, 2009Document50 pagesNP Outreach Curriculum in Rheumatology St. Joseph's Health Care, London, ON Dr. Sherry Rohekar November 12, 2009lynkx864100% (1)
- Arterial DisordersDocument40 pagesArterial DisordersSalman KhanNo ratings yet
- Pre Hand WritingDocument22 pagesPre Hand WritingIan Russ BautistaNo ratings yet
- Autoimmune DiseasesDocument125 pagesAutoimmune DiseasesJustin Ahorro-DionisioNo ratings yet
- Pediatric Hematooncology Alarm SymptomsDocument22 pagesPediatric Hematooncology Alarm SymptomsMuhammad ArifNo ratings yet
- Back PainDocument110 pagesBack PainRushdaNo ratings yet
- Prepared By: Madi, Krister: Salvador, Ma. Grace BSN-4ADocument36 pagesPrepared By: Madi, Krister: Salvador, Ma. Grace BSN-4ATap Tap100% (2)
- Sports Injuries and PreventionDocument43 pagesSports Injuries and PreventionDonajei RicaNo ratings yet
- Approach To Musculoskeletal SystemDocument18 pagesApproach To Musculoskeletal SystemdrgashokNo ratings yet
- Updated Activity Analysis Using The Occupational Therapy Practice Framework IIIDocument49 pagesUpdated Activity Analysis Using The Occupational Therapy Practice Framework IIIIan Russ Bautista100% (2)
- Rheumatology & Rehabilitation 2018-2019Document57 pagesRheumatology & Rehabilitation 2018-2019Selim TarekNo ratings yet
- Complex Regional Pain SyndromeDocument10 pagesComplex Regional Pain SyndromegeejeiNo ratings yet
- History Taking Orthopaedics CompleteDocument6 pagesHistory Taking Orthopaedics CompletenorisahnirishNo ratings yet
- Complex Regional Pain Syndrome: Pain Is An Unpleasant Sensory and Emotional ExperienceDocument34 pagesComplex Regional Pain Syndrome: Pain Is An Unpleasant Sensory and Emotional Experiencenitas23No ratings yet
- The Allen Cognitive Level Screen and The Allen BatteryDocument10 pagesThe Allen Cognitive Level Screen and The Allen BatteryIan Russ BautistaNo ratings yet
- Reflex Sympathetic DystrophyDocument32 pagesReflex Sympathetic DystrophyDelaram IravaniNo ratings yet
- AchillesDocument35 pagesAchillesNindyNo ratings yet
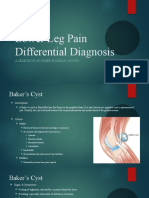
- Lower Leg Pain Differential Diagnosis - OtherDocument13 pagesLower Leg Pain Differential Diagnosis - Otherapi-619359087No ratings yet
- Peripheral Nerve DisordersDocument65 pagesPeripheral Nerve DisordersAdhityaRizkyPratamaNo ratings yet
- Numbness and HomoeopathyDocument32 pagesNumbness and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- 12C - Sudeck DystrophiaDocument12 pages12C - Sudeck DystrophiamorlaszloNo ratings yet
- Spinal Cord Injury (SCI) : Leads To DisabilityDocument30 pagesSpinal Cord Injury (SCI) : Leads To Disabilitymeli tswNo ratings yet
- Musculoskeletal Autoimmune Disorders: RA, SLE, SclerodermaDocument51 pagesMusculoskeletal Autoimmune Disorders: RA, SLE, SclerodermaSaya MenangNo ratings yet
- Ortho VIVA TopicsDocument22 pagesOrtho VIVA TopicsSiti RaudahNo ratings yet
- Indications and Contraindications 7 TherapyDocument14 pagesIndications and Contraindications 7 TherapyCecile SiauwNo ratings yet
- CTD1Document1 pageCTD1David HosamNo ratings yet
- Assessment and PT Management of STROKEDocument36 pagesAssessment and PT Management of STROKEAishwarya PanchalNo ratings yet
- Hypersensitivity and Autoimmune Disease: Kelompok 13 Fakultas Kedokteran Universitas LampungDocument23 pagesHypersensitivity and Autoimmune Disease: Kelompok 13 Fakultas Kedokteran Universitas LampungVictoria HawarimaNo ratings yet
- Osteoarthritis & Rheumatoid ArthritisDocument60 pagesOsteoarthritis & Rheumatoid ArthritisSaya MenangNo ratings yet
- Localising The Lesion Handout KateDocument13 pagesLocalising The Lesion Handout Katevtina177220No ratings yet
- Reflex Sympathetic Dystrophy andDocument37 pagesReflex Sympathetic Dystrophy andHarinderNo ratings yet
- Scleroderma, Sjogren's SyndromeDocument31 pagesScleroderma, Sjogren's SyndromeSalomeSibashviliNo ratings yet
- MF2 - Spinal Cord InjuryDocument43 pagesMF2 - Spinal Cord InjuryAnnbe BarteNo ratings yet
- 2 - MultipleSclerosisDocument32 pages2 - MultipleSclerosisHADI BADWANNo ratings yet
- Low back pain management and functional assessmentDocument76 pagesLow back pain management and functional assessmenthananNo ratings yet
- RHEUMATOID ARTHRITIS DR DON J SCOTT BERIN G BHMS (MEDICAL OFFICER) PDFDocument6 pagesRHEUMATOID ARTHRITIS DR DON J SCOTT BERIN G BHMS (MEDICAL OFFICER) PDFDr-Don JamesScott BerinGraceNo ratings yet
- Manual Therapy (Shs.405) : Dr. Muhamad Rizwan LecturerDocument28 pagesManual Therapy (Shs.405) : Dr. Muhamad Rizwan Lectureraad wwwNo ratings yet
- Medicine Seminar: Sakshi Malik 379 Shalini Singh 384 Sunanda Verma 394Document53 pagesMedicine Seminar: Sakshi Malik 379 Shalini Singh 384 Sunanda Verma 394966342No ratings yet
- Spinal TraumaDocument47 pagesSpinal TraumadeepaNo ratings yet
- Chapter 54 Assessment and Management of Patients With Rheumatic DisordersDocument19 pagesChapter 54 Assessment and Management of Patients With Rheumatic DisordersMaryrose GestosoNo ratings yet
- Aches and Pains in The Elderly: Diagnosis and TreatmentDocument34 pagesAches and Pains in The Elderly: Diagnosis and TreatmentAna CampeanuNo ratings yet
- Disorder of Musculo.system. Leatest PptxDocument178 pagesDisorder of Musculo.system. Leatest PptxCheru TecheNo ratings yet
- Spinal InjuryDocument40 pagesSpinal InjuryQuinnee VallejosNo ratings yet
- Vibration Disease EngDocument53 pagesVibration Disease EngVeronica SecrieruNo ratings yet
- Cumulative Trauma Disorders: Assessment and ManagementDocument57 pagesCumulative Trauma Disorders: Assessment and ManagementLeah DasNo ratings yet
- Rheumatic DiseasesDocument42 pagesRheumatic DiseasesToko RaMy LineNo ratings yet
- complicationsoffractures-120127084025-phpapp02-convertedDocument62 pagescomplicationsoffractures-120127084025-phpapp02-convertedAaliyah ShaikhNo ratings yet
- Of Physical Medicine & Rehabilitation, Marmara University, Istanbul TURKEY Mediterranean Forum of Physical Medicine and RehabilitationDocument46 pagesOf Physical Medicine & Rehabilitation, Marmara University, Istanbul TURKEY Mediterranean Forum of Physical Medicine and RehabilitationneareastspineNo ratings yet
- Soft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistDocument54 pagesSoft Tissue Disorders and Fibromyalgia: Jaya Ravindran Consultant RheumatologistarunupadhayaNo ratings yet
- Rheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderDocument53 pagesRheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderPande Indra PremanaNo ratings yet
- Multiple Sclerosis OfficialDocument20 pagesMultiple Sclerosis OfficialJerin XavierNo ratings yet
- Musculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersDocument51 pagesMusculoskeletal: Autoimmune Inflammatory Metabolic Infectious DisordersHarshoi KrishannaNo ratings yet
- Acute Compartment Syndrome in The Limbs: Presenter: Dr. Bulaya Moderator: Dr. WestDocument40 pagesAcute Compartment Syndrome in The Limbs: Presenter: Dr. Bulaya Moderator: Dr. Westhazunga rayfordNo ratings yet
- DOMMR Rheumatoid ArthritisDocument62 pagesDOMMR Rheumatoid Arthritisneeraj_bansal_3No ratings yet
- Rheumatology: - Syrian - Notes - CK - 2 - Step - Usmle - Pieces/8806 - Bits - CK - 2 - Step - Student - HTMLDocument5 pagesRheumatology: - Syrian - Notes - CK - 2 - Step - Usmle - Pieces/8806 - Bits - CK - 2 - Step - Student - HTMLLoyla RoseNo ratings yet
- Autoimmune Disorders: By: Kashif Qamar AfridiDocument24 pagesAutoimmune Disorders: By: Kashif Qamar Afridikashmala afzalNo ratings yet
- Unit 4 Study Guide Part 2Document7 pagesUnit 4 Study Guide Part 2NursingSchoolNotesNo ratings yet
- Multiple Sclerosis StudentDocument9 pagesMultiple Sclerosis StudentKelly WaskoNo ratings yet
- Medicine Yr3 NotesDocument3 pagesMedicine Yr3 Notesismah_haron_1No ratings yet
- Multiple Slerosis: Presented by HARSHA.JDocument43 pagesMultiple Slerosis: Presented by HARSHA.JAgatha SharmaNo ratings yet
- Uremic Encephalopathy: Causes, Symptoms and TreatmentDocument30 pagesUremic Encephalopathy: Causes, Symptoms and TreatmentRAechelle_Marc_4102No ratings yet
- Editable Gross Motor Skills Match and Move GameDocument6 pagesEditable Gross Motor Skills Match and Move GameIan Russ BautistaNo ratings yet
- Theories of Personality and PsychopathologyDocument68 pagesTheories of Personality and PsychopathologyIan Russ BautistaNo ratings yet
- Psychiatry: Human Development Throughout The Life CycleDocument64 pagesPsychiatry: Human Development Throughout The Life CycleIan Russ BautistaNo ratings yet
- Feeling Worksheet 7Document1 pageFeeling Worksheet 7Ian Russ BautistaNo ratings yet
- Psychiatry: Contributions of The Psychosocial Sciences To Human BehaviorDocument35 pagesPsychiatry: Contributions of The Psychosocial Sciences To Human BehaviorIan Russ BautistaNo ratings yet
- Psychiatry Tests Guide Intelligence and PersonalityDocument17 pagesPsychiatry Tests Guide Intelligence and PersonalityIan Russ BautistaNo ratings yet
- Chemical Basis of Life 2Document3 pagesChemical Basis of Life 2Ian Russ BautistaNo ratings yet
- Genchemlab Expt. 10 Acids and BasesDocument5 pagesGenchemlab Expt. 10 Acids and BasesIan Russ BautistaNo ratings yet
- SacramentDocument38 pagesSacramentIan Russ BautistaNo ratings yet
- ANA1Lab of Shoulder and Scapula - Student GuideDocument9 pagesANA1Lab of Shoulder and Scapula - Student GuideIan Russ BautistaNo ratings yet
- Data Extraction Tool Ni AyniDocument7 pagesData Extraction Tool Ni AyniIan Russ BautistaNo ratings yet
- ROL Summary Table EDITED Ni AyniDocument12 pagesROL Summary Table EDITED Ni AyniIan Russ BautistaNo ratings yet
- Hello WorldDocument1 pageHello WorldIan Russ BautistaNo ratings yet