You might also like
- Borders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudiesDocument22 pagesBorders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudieskarmayagnaNo ratings yet
- Spiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerDocument16 pagesSpiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerkarmayagnaNo ratings yet
- BhagavadGita theArtofLeadership OldTextNewContextDocument19 pagesBhagavadGita theArtofLeadership OldTextNewContextkarmayagnaNo ratings yet
- Manufacturing Process MapDocument1 pageManufacturing Process MapkarmayagnaNo ratings yet
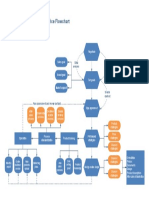
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaNo ratings yet
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDocument1 pageFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaNo ratings yet
- Flow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchDocument1 pageFlow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchkarmayagnaNo ratings yet
- Order FlowchartDocument1 pageOrder FlowchartkarmayagnaNo ratings yet
- Beer Processing PFDDocument1 pageBeer Processing PFDkarmayagnaNo ratings yet
- Secondary Orbital MlanomasDocument5 pagesSecondary Orbital MlanomaskarmayagnaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ch42 NCP IneffectiveCoping 1075-1076Document2 pagesCh42 NCP IneffectiveCoping 1075-1076Jane GarciaNo ratings yet
- Review of CA' Dept of Behavioral Health PDFDocument466 pagesReview of CA' Dept of Behavioral Health PDFRoxanne ReevesNo ratings yet
- Healing Architecture: A Spatial Experience Praxis: Khaled Sayed AsfourDocument15 pagesHealing Architecture: A Spatial Experience Praxis: Khaled Sayed AsfourKatherine La Torre CayetanoNo ratings yet
- Respiratory Distress Syndrome LapkasDocument49 pagesRespiratory Distress Syndrome LapkasThamarai SomuNo ratings yet
- Glaukoma - PPTX KoassDocument38 pagesGlaukoma - PPTX Koassdhita01No ratings yet
- Differential Diagnosis of PULMONARY EDEMADocument3 pagesDifferential Diagnosis of PULMONARY EDEMAHY Hong YiNo ratings yet
- Borderline Personality DisorderDocument25 pagesBorderline Personality DisordersindhurajNo ratings yet
- Constipation NCPDocument2 pagesConstipation NCPjudaperlNo ratings yet
- Residential Care Quick Facts Directory 2017Document600 pagesResidential Care Quick Facts Directory 2017Tyler Harper100% (1)
- Colour Therapy - Supra PowDocument7 pagesColour Therapy - Supra PowrkNo ratings yet
- What Clexane Is and What It Is Used For How To Use ClexaneDocument2 pagesWhat Clexane Is and What It Is Used For How To Use ClexaneAruna KaranamNo ratings yet
- Celsite, Surecan, Cytocan: Access Port Systems, Piccs, Accessories and Non-Coring Port NeedlesDocument36 pagesCelsite, Surecan, Cytocan: Access Port Systems, Piccs, Accessories and Non-Coring Port NeedlesmochkurniawanNo ratings yet
- Woman Undergoes Revolutionary Treatment For Her Lifelong DepressionDocument2 pagesWoman Undergoes Revolutionary Treatment For Her Lifelong DepressionsarahnorrisNo ratings yet
- DR SabaDocument2 pagesDR SabaMuhammad Abrar YousafzaiNo ratings yet
- Life Mapping Templates v1Document4 pagesLife Mapping Templates v1Maria Mastroianni100% (1)
- Massage Therapy Research Review PDFDocument30 pagesMassage Therapy Research Review PDFIne Marthia DanieNo ratings yet
- Hypoglycaemia Documented With Real-Time Continuous Glucose Sensing in A Case of Dead in Bed' SyndromeDocument106 pagesHypoglycaemia Documented With Real-Time Continuous Glucose Sensing in A Case of Dead in Bed' Syndromemimran1974No ratings yet
- Plant Usage in Protecting The Farm Animal Health - V. Davidović, M. Joksimović Todorović, B. Stojanović, R. RelićDocument12 pagesPlant Usage in Protecting The Farm Animal Health - V. Davidović, M. Joksimović Todorović, B. Stojanović, R. RelićCk_psihNo ratings yet
- 13 IMPLANT SUPPORTED FIXED PROSTHESESmic PDFDocument52 pages13 IMPLANT SUPPORTED FIXED PROSTHESESmic PDFManaila GeorgianNo ratings yet
- C AnnulationDocument15 pagesC AnnulationSaffronMaeNo ratings yet
- Acute Vs Chronic Renal Failure.Document3 pagesAcute Vs Chronic Renal Failure.Stephanie HurewitzNo ratings yet
- ResearchDocument11 pagesResearchRheagin GumbanNo ratings yet
- BPSY 50 Ch1 Introduction To PsychologyDocument2 pagesBPSY 50 Ch1 Introduction To PsychologyKatherine SapoNo ratings yet
- Ghanbari HamidDocument2 pagesGhanbari Hamidapi-256797118No ratings yet
- Ominous Octet For PharmacistsDocument16 pagesOminous Octet For PharmaciststreeshadowNo ratings yet
- 'NEXtCARE Egypt - Reimbursement FormDocument1 page'NEXtCARE Egypt - Reimbursement FormMohyee Eldin RagebNo ratings yet
- Stability of The Ready-To-Use Solutions of Eribulin For Intravenous InfusionDocument7 pagesStability of The Ready-To-Use Solutions of Eribulin For Intravenous InfusionKinesh PatelNo ratings yet
- Aaron T Beck TranscriptDocument21 pagesAaron T Beck TranscriptcorsovaNo ratings yet
- Report - Language and The BrainDocument38 pagesReport - Language and The BrainBryanNo ratings yet
- Iliotibial Band Syndrome - FannyDocument13 pagesIliotibial Band Syndrome - FannyAlfiani Rosyida Arisanti Syafi'iNo ratings yet