You might also like
- BhagavadGita theArtofLeadership OldTextNewContextDocument19 pagesBhagavadGita theArtofLeadership OldTextNewContextkarmayagnaNo ratings yet
- Spiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerDocument16 pagesSpiritual Development Through The Chakra Progression: Jennifer Drapkin, Clayton Mcclintock, Elsa Lau, Lisa MillerkarmayagnaNo ratings yet
- Borders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudiesDocument22 pagesBorders Crossed: Vibhishana in The Ramayana and Beyond: South Asia: Journal of South Asian StudieskarmayagnaNo ratings yet
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDocument1 pageFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaNo ratings yet
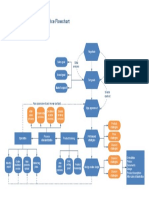
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaNo ratings yet
- Manufacturing WorkflowDocument1 pageManufacturing WorkflowDidik HariadiNo ratings yet
- Manufacturing Process MapDocument1 pageManufacturing Process MapkarmayagnaNo ratings yet
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaNo ratings yet
- Beer Production ProcessDocument1 pageBeer Production ProcesskarmayagnaNo ratings yet
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaNo ratings yet
- Manufacturing Process MapDocument1 pageManufacturing Process MapkarmayagnaNo ratings yet
- Flowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupsDocument1 pageFlowchart of The Industrial Process For The Manufacturing of Plastic Yogurt CupskarmayagnaNo ratings yet
- Beer Processing PFDDocument1 pageBeer Processing PFDkarmayagnaNo ratings yet
- Main Functions of The Operative Manufacturing Execution LevelDocument1 pageMain Functions of The Operative Manufacturing Execution LevelkarmayagnaNo ratings yet
- Flow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchDocument1 pageFlow Chart of The Manufacturing Process Used by Arena Software Numbers Indicating BatchkarmayagnaNo ratings yet
- Logical Flow Diagram of The Production Process OperationsDocument1 pageLogical Flow Diagram of The Production Process OperationskarmayagnaNo ratings yet
- Intra Arterial ChemotherapyDocument6 pagesIntra Arterial ChemotherapykarmayagnaNo ratings yet
- Oral CancerDocument5 pagesOral CancerkarmayagnaNo ratings yet
- Order WorkflowDocument1 pageOrder WorkflowkarmayagnaNo ratings yet
- Server WorkflowDocument1 pageServer WorkflowkarmayagnaNo ratings yet
- Outcome of SQ .Cell CA of GingivaDocument5 pagesOutcome of SQ .Cell CA of GingivakarmayagnaNo ratings yet
- Services FlowchartDocument1 pageServices FlowchartLuis Fernando Sanchez TapiaNo ratings yet
- Quality Control Process: Material SupplierDocument1 pageQuality Control Process: Material Supplieralva10 vaNo ratings yet
- Manufacturing WorkflowDocument1 pageManufacturing WorkflowDidik HariadiNo ratings yet
- Order FlowchartDocument1 pageOrder FlowchartkarmayagnaNo ratings yet
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaNo ratings yet
- Relationship of Tumor Thickness in Punch Biopsy and SubsequentDocument4 pagesRelationship of Tumor Thickness in Punch Biopsy and SubsequentkarmayagnaNo ratings yet
- Secondary Orbital MlanomasDocument5 pagesSecondary Orbital MlanomaskarmayagnaNo ratings yet
- Survival After Oral CancerDocument5 pagesSurvival After Oral CancerkarmayagnaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Province Wise List of MVCS, Cvcs and Avcs: District Tehsil HF Name Address Contact No TimingsDocument37 pagesProvince Wise List of MVCS, Cvcs and Avcs: District Tehsil HF Name Address Contact No TimingsAbdullah AbdullahNo ratings yet
- Dark Psychology and Manipulation by Richard CovertDocument129 pagesDark Psychology and Manipulation by Richard CovertAteng Ph100% (1)
- Grp4 Act1 Disaster Nursing LabDocument5 pagesGrp4 Act1 Disaster Nursing Labaaron tabernaNo ratings yet
- Orthopaedic Fellowships in India After PGDocument4 pagesOrthopaedic Fellowships in India After PGNEPDOC OFFICIAL100% (1)
- The Information Effect ProjectDocument3 pagesThe Information Effect Projectapi-365448428No ratings yet
- Occupational Health and HygieneDocument40 pagesOccupational Health and HygieneAISYAH NABILAH ROSLANNo ratings yet
- Hazardous Materials and Wastes Management PlanDocument5 pagesHazardous Materials and Wastes Management Planaloysius akpanNo ratings yet
- Time To Synergize Mental Health With Brain Health: CommentDocument3 pagesTime To Synergize Mental Health With Brain Health: Commentsoliveira_149796No ratings yet
- Cook Poultry and Game DishesDocument7 pagesCook Poultry and Game DishesJohn Michael ItableNo ratings yet
- ReDoc Sample SLP Reports PedsDocument16 pagesReDoc Sample SLP Reports PedsXlian Myzter YosaNo ratings yet
- PSFO - Tip Sheet - Eye-Hand CoordinationDocument2 pagesPSFO - Tip Sheet - Eye-Hand Coordinationharem bakirNo ratings yet
- Fluent League of Legends - Advanced Wave ManagementDocument35 pagesFluent League of Legends - Advanced Wave ManagementSteveyBreekiNo ratings yet
- The Effect of Jazz Music on Undergraduate Students' CreativityDocument3 pagesThe Effect of Jazz Music on Undergraduate Students' CreativityROSE ANN LOPERANo ratings yet
- Market Reflection Report AUG'22Document23 pagesMarket Reflection Report AUG'22Komal RaneNo ratings yet
- StockKamis30Juli'20 PBF. SMSDocument24 pagesStockKamis30Juli'20 PBF. SMSAiko Cheryl SalsabilaNo ratings yet
- 5697483-01 CARESCAPE Canvas S A SUPPL v3-3 ENG INTLDocument33 pages5697483-01 CARESCAPE Canvas S A SUPPL v3-3 ENG INTLJef RobinsonNo ratings yet
- Pedia History Taking (Oct9)Document5 pagesPedia History Taking (Oct9)fall autumnNo ratings yet
- Cost Benefit Analysis Concepts and Practice 5th Edition Boardman Test BankDocument26 pagesCost Benefit Analysis Concepts and Practice 5th Edition Boardman Test BankMelissaBakerijgd96% (56)
- Apr 78Document147 pagesApr 78Quality AssuranceNo ratings yet
- Nursing Cover LetterDocument1 pageNursing Cover Letterapi-365022171No ratings yet
- New Recommendations According To 2022 ILCOR CoSTDocument1 pageNew Recommendations According To 2022 ILCOR CoSTMineTagraNo ratings yet
- Ohsas 18001Document2 pagesOhsas 18001Tarek FawzyNo ratings yet
- 4 Virtues Emanating From The Practice of CharityDocument2 pages4 Virtues Emanating From The Practice of CharityMykristie Jho B. MendezNo ratings yet
- Eysenck Personality Inventory (EPI) SCALEDocument4 pagesEysenck Personality Inventory (EPI) SCALEchinna duraiNo ratings yet
- Case Study Acute Myocardial InfarctionDocument11 pagesCase Study Acute Myocardial InfarctionChristine Elaine Batusin Ilagan91% (23)
- Recipe Modification for Sodium Control Case StudyDocument1 pageRecipe Modification for Sodium Control Case StudyKaitlyn BretoiNo ratings yet
- Multiple Role Conflict Faced by WomenDocument14 pagesMultiple Role Conflict Faced by WomenmnhassenmnhNo ratings yet
- Physical Education and Health Flexible Instruction Delivery PlanDocument4 pagesPhysical Education and Health Flexible Instruction Delivery PlanAngelyn Lingatong67% (3)
- Physical Development of InfantsDocument4 pagesPhysical Development of InfantsJefferson SociasNo ratings yet
- Demographic terms definedDocument11 pagesDemographic terms definedkasoziNo ratings yet