You might also like
- Nursing Care Plan For HypertensionDocument2 pagesNursing Care Plan For HypertensionFranco Razon100% (1)
- Nursing Care Plan For HypertensionDocument5 pagesNursing Care Plan For Hypertensionmariejo89% (81)
- NCP Hypertension 2Document3 pagesNCP Hypertension 2Roseben Somido50% (2)
- Diabetic Patient with Pre-eclampsiaDocument2 pagesDiabetic Patient with Pre-eclampsiaJen Faye Orpilla100% (9)
- Managing Hypertension and Decreased Cardiac OutputDocument5 pagesManaging Hypertension and Decreased Cardiac Outputanon_9189425950% (2)
- Nursing Care PlanDocument9 pagesNursing Care PlanLura Xstilice B. Galinato100% (1)
- Nursing Care PlanDocument10 pagesNursing Care PlanZerica Andaca83% (6)
- Anemia Nursing Care PlanDocument3 pagesAnemia Nursing Care PlanRosita HutamiNo ratings yet
- NCP For HypertensionDocument4 pagesNCP For HypertensionCiariz Charisse83% (6)
- Nursing Care Plan For HypoglycemiaDocument3 pagesNursing Care Plan For HypoglycemiaCyrus De Asis83% (53)
- Nursing Care Plan For HypertensionDocument3 pagesNursing Care Plan For HypertensionFranco Razon100% (2)
- Improve Activity Tolerance and Manage Nursing DiagnosesDocument14 pagesImprove Activity Tolerance and Manage Nursing DiagnosesIbrahimWages100% (4)
- Nursing Care PlanDocument37 pagesNursing Care Planpia lestrange100% (6)
- Nursing Care Plan Congestive Heart FailureDocument2 pagesNursing Care Plan Congestive Heart FailureRalph Dumawaa60% (5)
- Hypertension Mini Case StudyDocument5 pagesHypertension Mini Case Studymaeca101100% (1)
- NURSING CARE PLAN For Myocardial InfarctionDocument16 pagesNURSING CARE PLAN For Myocardial InfarctionFreisanChenMandumotan100% (1)
- "Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Nursing Care PlansDocument21 pages"Acute Coronary Syndrome Non ST Elevation Myocardial Infarction, Hypertensive Cardiovascular Disease, Diabetes Mellitus Type 2, and Community Acquired Pneumonia" Nursing Care PlansCarl Elexer Cuyugan Ano100% (1)
- NCP HypertensionDocument2 pagesNCP Hypertensionsinister1781% (27)
- Nursing Care Plan "Diabetes"Document8 pagesNursing Care Plan "Diabetes"Senor SeniorNo ratings yet
- Nursing Care Plan For "Heart Failure Chronic"Document16 pagesNursing Care Plan For "Heart Failure Chronic"jhonroks97% (34)
- Hypertension Nursing Care PlanDocument2 pagesHypertension Nursing Care PlanCyrus De Asis92% (13)
- Nursing Care Plan For Angina Pectoris NCPDocument2 pagesNursing Care Plan For Angina Pectoris NCPderic73% (15)
- Nursing Care Plan HypertensionDocument2 pagesNursing Care Plan Hypertensionderic98% (124)
- Nursing Care Plans for Acute Pain, Hyperthermia, Activity Intolerance, and Infection RiskDocument20 pagesNursing Care Plans for Acute Pain, Hyperthermia, Activity Intolerance, and Infection RiskNursidar Pascual Mukattil80% (5)
- Care Plan Prep May 13 Rheumatic FeverDocument16 pagesCare Plan Prep May 13 Rheumatic Feverapi-256360167No ratings yet
- ACS Nursing Care PlanDocument21 pagesACS Nursing Care Planchris_arc90100% (6)
- Diabetes Mellitus Nursing Care PlanDocument7 pagesDiabetes Mellitus Nursing Care PlanjamieboyRN90% (31)
- Nursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Document3 pagesNursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Kenneth Anthony Tiu Regida100% (8)
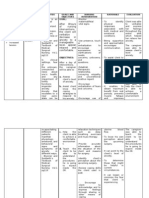
- Cues/ Data Goal of Care Objectives of Care Nursing Intervention Rationale Method of Family Contact Resources Required EvaluationDocument2 pagesCues/ Data Goal of Care Objectives of Care Nursing Intervention Rationale Method of Family Contact Resources Required EvaluationKhleanne CastilloNo ratings yet
- Defining Characteristics: ConfusionDocument12 pagesDefining Characteristics: ConfusionGio LlanosNo ratings yet
- Nursing Care Plan for AnxietyDocument2 pagesNursing Care Plan for AnxietyMelinda Cariño BallonNo ratings yet
- Gerontologic NCPDocument8 pagesGerontologic NCPLouren Grace Quinto AnceroNo ratings yet
- Disturbed Thought Process Related CNS Infection by HIVDocument5 pagesDisturbed Thought Process Related CNS Infection by HIVNatukunda DianahNo ratings yet
- H.C. Risk Factors and Nursing Care PlanDocument4 pagesH.C. Risk Factors and Nursing Care PlanMary Hope Bacuta0% (2)
- Barecuatro Module1 NCP2Document4 pagesBarecuatro Module1 NCP2ANGELICA CLAIRE BARECUATRONo ratings yet
- The Patient%u2019s Experience With Critical IllnessDocument15 pagesThe Patient%u2019s Experience With Critical IllnessineNo ratings yet
- Ha Lec Prelim 2Document2 pagesHa Lec Prelim 2Hershey VilladelgadoNo ratings yet
- NCP, 3 Case StudyDocument9 pagesNCP, 3 Case StudyKrishelle Kate PannigNo ratings yet
- Nursing Analysis, Goals and Rationale for AnxietyDocument2 pagesNursing Analysis, Goals and Rationale for AnxietyIris Coronel AdamosNo ratings yet
- Introduction To Health AssessmentDocument5 pagesIntroduction To Health AssessmentHanna BuadaNo ratings yet
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- Nursing assessment diagnosis interventions rationale evaluationDocument3 pagesNursing assessment diagnosis interventions rationale evaluationanimesh pandaNo ratings yet
- NCP of Endometrical CancerDocument2 pagesNCP of Endometrical CancerFrando kennethNo ratings yet
- Family Nursing Care Plan for Hypertension and Coronary Artery DiseaseDocument3 pagesFamily Nursing Care Plan for Hypertension and Coronary Artery DiseaseKrizzia Mae F. MayoresNo ratings yet
- Sample NCPDocument3 pagesSample NCPJoedelynne Diane Endaya GarciaNo ratings yet
- NCP (Gonzales) Mar 29 - Ventura PDFDocument3 pagesNCP (Gonzales) Mar 29 - Ventura PDFJian VenturaNo ratings yet
- Schizophrenia Paranoid Type Nursing CareDocument2 pagesSchizophrenia Paranoid Type Nursing CareKervy JuntillaNo ratings yet
- Ineffective Coping - Nursing Diagnosis & Care Plan - NurseslabsDocument13 pagesIneffective Coping - Nursing Diagnosis & Care Plan - NurseslabsLester MooreNo ratings yet
- Pathophysiology and Nursing Interventions for ObesityDocument6 pagesPathophysiology and Nursing Interventions for ObesitySummer pickNo ratings yet
- Asuhan Keperawatan GerontikDocument13 pagesAsuhan Keperawatan GerontikEnggal PratamaNo ratings yet
- Anxiety: Generalized Anxiety Disorder Assessment (Behavioral Health) - CEDocument7 pagesAnxiety: Generalized Anxiety Disorder Assessment (Behavioral Health) - CEircomfarNo ratings yet
- Concept of PsychoeducationDocument22 pagesConcept of PsychoeducationAli100% (3)
- Tuano, Salma M. Bsn4-1 Fear/AnxietyDocument3 pagesTuano, Salma M. Bsn4-1 Fear/AnxietySALMA M. TUANO100% (1)
- Chapter 10 Basic Features of Clinical InterventionDocument3 pagesChapter 10 Basic Features of Clinical InterventionKathleenNicole De Castro EnfectanaNo ratings yet
- St. Anthony's College Nursing DepartmentDocument6 pagesSt. Anthony's College Nursing DepartmentKalix JaceNo ratings yet
- Acute PainDocument4 pagesAcute PainRuffy AbdulazisNo ratings yet
- RNSG2160 Mental Health Clinical Concept MapDocument2 pagesRNSG2160 Mental Health Clinical Concept MapRhina FutrellNo ratings yet
- Generalized Anxiety DisorderDocument24 pagesGeneralized Anxiety DisorderEula Angelica OcoNo ratings yet
- Good Resource!! ConditionsDocument288 pagesGood Resource!! Conditionsizzy jusufi100% (1)
- General Principles and Empirically Supported Techniques of Cognitive Behavior TherapyFrom EverandGeneral Principles and Empirically Supported Techniques of Cognitive Behavior TherapyNo ratings yet
- ShockDocument5 pagesShockJowzefNo ratings yet
- Abortion Write UpDocument3 pagesAbortion Write UpJowzef100% (1)
- New Consultant CompanyDocument51 pagesNew Consultant CompanyJowzefNo ratings yet
- ShockDocument5 pagesShockJowzefNo ratings yet
- 03 Entrepren ch4Document38 pages03 Entrepren ch4JowzefNo ratings yet
- Paed Case #2Document5 pagesPaed Case #2JowzefNo ratings yet
- Psychological Factors Causing Mental IllnessDocument5 pagesPsychological Factors Causing Mental IllnessJowzefNo ratings yet
- Lecture Notes Part1Document29 pagesLecture Notes Part1JowzefNo ratings yet
- Jowzef Community Health NursingDocument5 pagesJowzef Community Health NursingJowzefNo ratings yet
- Low Birth WeightDocument1 pageLow Birth WeightJowzef100% (1)
- Medical Surgical Nursing An Integrated Approach 3rd Edition White Test BankDocument12 pagesMedical Surgical Nursing An Integrated Approach 3rd Edition White Test Bankpauldiamondwe8100% (27)
- CAP Protocol-2016 Thyroid - HighlightedDocument8 pagesCAP Protocol-2016 Thyroid - Highlightedpath2016No ratings yet
- PosterDocument3 pagesPosterMadel Tutor ChaturvediNo ratings yet
- Setting up MRI Scan CentresDocument86 pagesSetting up MRI Scan CentresGokilavani RajagopalNo ratings yet
- Blood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationDocument2 pagesBlood Agar Base (Infusion Agar) : Intended Use Summary and ExplanationSarehElizabetNo ratings yet
- Analgesia en Dolor Ciático Agudo Con La Cauterización Del Punto Ciático AuricularDocument68 pagesAnalgesia en Dolor Ciático Agudo Con La Cauterización Del Punto Ciático Auricularsoyunchingon1100% (1)
- Heinz Kohut - Self PsychologyDocument49 pagesHeinz Kohut - Self PsychologyDesiree Pescasio DimasuayNo ratings yet
- Internal Medicine 5th MidtermDocument13 pagesInternal Medicine 5th MidtermIashdip iashdipNo ratings yet
- COVID-19 Vaccination Certificate from India's Ministry of HealthDocument1 pageCOVID-19 Vaccination Certificate from India's Ministry of Healthbliss bNo ratings yet
- Prak Ospe PK FMS 3 2021Document7 pagesPrak Ospe PK FMS 3 2021Angelique NatalieNo ratings yet
- Disorder and Diseases of Digestive SystemDocument8 pagesDisorder and Diseases of Digestive SystemCristina AnganganNo ratings yet
- Migraine DiagnosisDocument7 pagesMigraine DiagnosisMariaAmeliaGoldieNo ratings yet
- Cardiovascular System (CVS) - Ii: MBBS Year-3 (Academic Year 2020-2021)Document10 pagesCardiovascular System (CVS) - Ii: MBBS Year-3 (Academic Year 2020-2021)FarsibalooNo ratings yet
- Klenner Protocol For 2013Document10 pagesKlenner Protocol For 2013jcoppala4476No ratings yet
- Sorbitol Side Effects, Dosages and WarningsDocument7 pagesSorbitol Side Effects, Dosages and Warningskuya batokNo ratings yet
- Keto DietDocument2 pagesKeto DietdewiNo ratings yet
- Certificate of Accreditation: Swift Silliker (Pty) LTDDocument10 pagesCertificate of Accreditation: Swift Silliker (Pty) LTDpham xuan tinh tinhNo ratings yet
- Keratoconus An Inflamatory DisorderDocument17 pagesKeratoconus An Inflamatory DisorderNATALIA CARMONA REYESNo ratings yet
- Cardiovascular System AgingDocument17 pagesCardiovascular System Agingapi-541796556No ratings yet
- Lesson Plan Health 7Document4 pagesLesson Plan Health 7Arlene74% (23)
- Kuliah Biokimia-Imunokimia FK UNDIPDocument19 pagesKuliah Biokimia-Imunokimia FK UNDIPPutri HapsariNo ratings yet
- Disneynature's Chimpanzee Educator's GuideDocument135 pagesDisneynature's Chimpanzee Educator's GuideNaomi ShapiroNo ratings yet
- Unveiling Tetanus A Comprehensive Exploration of The Causes Symptoms Prevention and TreatmentDocument12 pagesUnveiling Tetanus A Comprehensive Exploration of The Causes Symptoms Prevention and TreatmentMikhil mchaeladdictionsNo ratings yet
- Camca Prelim Reviewer 2Document11 pagesCamca Prelim Reviewer 2Danna MedranaNo ratings yet
- Controlling Fluid Intake in Heart FailureDocument3 pagesControlling Fluid Intake in Heart FailureNavojit ChowdhuryNo ratings yet
- Unit 2 Blood - Body BitsDocument3 pagesUnit 2 Blood - Body BitsJohnny Miller60% (5)
- What Is A Urinary Tract InfectionDocument3 pagesWhat Is A Urinary Tract InfectionStepyn SalvadorNo ratings yet
- Detoxification of Pesticide Waste Via Activated Carbon Adsorption ProcessDocument11 pagesDetoxification of Pesticide Waste Via Activated Carbon Adsorption ProcessNadia MandasariNo ratings yet
- Ave Lox TabsDocument5 pagesAve Lox Tabslrdn_ghrcNo ratings yet