You might also like
- 2008 ExpenseDocument1 page2008 Expensepamela_talley2806No ratings yet
- "Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsDocument2 pages"Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsButtNo ratings yet
- Weekly Report Template - Expense ReportDocument2 pagesWeekly Report Template - Expense ReportMOHAMEDNo ratings yet
- Expense Report: Company NameDocument2 pagesExpense Report: Company NameMOHAMEDNo ratings yet
- Expense SheetDocument3 pagesExpense SheetMuntaser AlrefaiNo ratings yet
- "Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsDocument2 pages"Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsButtNo ratings yet
- Corporate Pay Stub Template-PDF Reader ProDocument1 pageCorporate Pay Stub Template-PDF Reader ProUmar AliNo ratings yet
- Monthly Budget Worksheet: HousingDocument3 pagesMonthly Budget Worksheet: HousingrizviNo ratings yet
- Travel ReimbDocument1 pageTravel ReimbThe APA Division of PsychotherapyNo ratings yet
- HR expenses Q1-Q4 reportDocument1 pageHR expenses Q1-Q4 reportRaj Kothari MNo ratings yet
- Mileage Report DateDocument1 pageMileage Report DateSpencer MarstonNo ratings yet
- Construction ProposalDocument2 pagesConstruction ProposalzaidNo ratings yet
- Expense Report: (Insert Company Logo)Document4 pagesExpense Report: (Insert Company Logo)HOSAM HUSSEINNo ratings yet
- CHurch BudgetDocument2 pagesCHurch BudgetdeycallmebudNo ratings yet
- ExpRep-21Document1 pageExpRep-21Anonymous 1aRDJO4VeNo ratings yet
- IC Hourly Invoice Template GoogleDocument3 pagesIC Hourly Invoice Template GoogleThanh NguyenNo ratings yet
- "Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsDocument8 pages"Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsButtNo ratings yet
- Construction Quote TemplateDocument2 pagesConstruction Quote Templateshivraj bankarNo ratings yet
- Construction Quote 1Document2 pagesConstruction Quote 1mNo ratings yet
- Quote Template 03Document2 pagesQuote Template 03victorNo ratings yet
- Mohamed MahdiDocument5 pagesMohamed Mahdimohamed khadarNo ratings yet
- Receipt 29sep2023 202750Document1 pageReceipt 29sep2023 202750Daniel TeixeiraNo ratings yet
- Income and Expense TEMPLATEDocument2 pagesIncome and Expense TEMPLATEDacia Bolton BatesNo ratings yet
- About This TemplateDocument2 pagesAbout This Templateapi-658027506No ratings yet
- Hotel Daily Sales ReportDocument5 pagesHotel Daily Sales ReportSatu Dua Coffee & RestoNo ratings yet
- Invoice Template 5 WordDocument2 pagesInvoice Template 5 WordGuardian Network BangladeshNo ratings yet
- BillsDocument2 pagesBillsraju chintapatlaNo ratings yet
- Leslie Ha Contract Quote PDFDocument1 pageLeslie Ha Contract Quote PDFfllamas1973No ratings yet
- Rommmate BudgetDocument3 pagesRommmate Budgetapi-339459052No ratings yet
- Rommmate BudgetDocument3 pagesRommmate Budgetapi-339307202No ratings yet
- Budget Large ConferenceDocument3 pagesBudget Large ConferencefarhanNo ratings yet
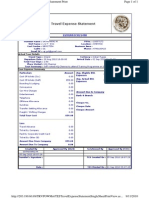
- Travel Expense Statement PrintDocument1 pageTravel Expense Statement PrintdoubleffNo ratings yet
- Simple personal budgetDocument3 pagesSimple personal budgetTeddy GutayNo ratings yet
- InvoiceforLBR 591849128482539Document1 pageInvoiceforLBR 591849128482539Princess InfornonNo ratings yet
- Classic Word Invoice TemplateDocument1 pageClassic Word Invoice TemplateKwartirranting BengkongNo ratings yet
- Presupuesto Mensual PersonalDocument2 pagesPresupuesto Mensual PersonalCarlos MaldonadoNo ratings yet
- Jessica PayslipDocument2 pagesJessica Payslipdavd brebNo ratings yet
- InvoiceDocument1 pageInvoiceTatar EdhyNo ratings yet
- Courier Invoice TemplateDocument1 pageCourier Invoice Templatehannah aileen fernandezNo ratings yet
- Name of Agency Here: Part 1: Monthly Income Estimated ActualDocument1 pageName of Agency Here: Part 1: Monthly Income Estimated ActualFaith MarcathyNo ratings yet
- Your Logo: Sample Construction Work Order TemplateDocument2 pagesYour Logo: Sample Construction Work Order TemplatesaalihNo ratings yet
- Fred Keller April 2011 Expense ReportDocument1 pageFred Keller April 2011 Expense ReportPAHouseGOPNo ratings yet
- Monthly Budget Tracker1Document2 pagesMonthly Budget Tracker1mark uchihaNo ratings yet
- Monthly BudjetDocument2 pagesMonthly BudjetA Wahid KemalNo ratings yet
- Mahalaxmi Prasad CHS April billsDocument45 pagesMahalaxmi Prasad CHS April billsssandeepNo ratings yet
- Invoice Template for Your Company NameDocument1 pageInvoice Template for Your Company NameTatar EdhyNo ratings yet
- Property Tax BillDocument2 pagesProperty Tax Billdipan.routNo ratings yet
- Travel Service Invoice1Document1 pageTravel Service Invoice1Labinot DemiNo ratings yet
- "Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsDocument21 pages"Untitled Austin Project": Crown Venice Productions, LLC ReimbursementsButtNo ratings yet
- Contoh InvoiceDocument2 pagesContoh InvoiceFATAHILLAH SHOLAHUDDINSWARDANINo ratings yet
- Blank Yearly Budget Plan TemplateDocument1 pageBlank Yearly Budget Plan TemplateianachieviciNo ratings yet
- About This TemplateDocument2 pagesAbout This TemplatearsocialidNo ratings yet
- Nats-Income StatementDocument1 pageNats-Income Statementapi-251378367No ratings yet
- About This TemplateDocument3 pagesAbout This TemplateKhánh ĐặngNo ratings yet
- Description Weekly Fortnightly Monthly Quarterly Bi-Annual AnnualDocument2 pagesDescription Weekly Fortnightly Monthly Quarterly Bi-Annual Annualrosy ranaNo ratings yet
- Invoice Template 4 WordDocument1 pageInvoice Template 4 WordRykad Computer solutionsNo ratings yet
- Adam Narrell Contract Quote PDFDocument1 pageAdam Narrell Contract Quote PDFfllamas1973No ratings yet
- The Good StewardDocument14 pagesThe Good StewardRibhararnus PracutiarNo ratings yet
- Nicl Exam GK Capsule: 25 March, 2015Document69 pagesNicl Exam GK Capsule: 25 March, 2015Jatin YadavNo ratings yet
- Alifian Faiz NovendiDocument5 pagesAlifian Faiz Novendialifianovendi 11No ratings yet
- GASODOR S-FreeDocument7 pagesGASODOR S-FreeDavid Jesus Mejias LlanosNo ratings yet
- CDP VasaivirarDocument194 pagesCDP VasaivirarKruti ShahNo ratings yet
- Tourism MarketingDocument27 pagesTourism MarketingJade Lyn LopezNo ratings yet
- Nestle Global Strategy Case Study AnalysisDocument16 pagesNestle Global Strategy Case Study AnalysisSameer Bin Sadaqat0% (1)
- Coffe Production in Colombia PDFDocument4 pagesCoffe Production in Colombia PDFJuanes RestrepoNo ratings yet
- Crop Insurance - BrazilDocument3 pagesCrop Insurance - Brazilanandekka84No ratings yet
- Josh Magazine NMAT 2007 Quest 4Document43 pagesJosh Magazine NMAT 2007 Quest 4Pristine Charles100% (1)
- Seminar Assignments Multiple Choice Questions City Size Growth PDFDocument4 pagesSeminar Assignments Multiple Choice Questions City Size Growth PDFminlwintheinNo ratings yet
- Regional Planning Techniques PDFDocument131 pagesRegional Planning Techniques PDFRicha Sagarika0% (1)
- Rethinking Monetary Policy After the CrisisDocument23 pagesRethinking Monetary Policy After the CrisisAlexDuarteVelasquezNo ratings yet
- MEC 1st Year 2020-21 EnglishDocument16 pagesMEC 1st Year 2020-21 EnglishKumar UditNo ratings yet
- Legal NoticeDocument7 pagesLegal NoticeRishyak BanavaraNo ratings yet
- Selected Bibliography On The Right To Development PDFDocument32 pagesSelected Bibliography On The Right To Development PDFMatheus GobbatoNo ratings yet
- Amb 336 Case Study AnalysisDocument10 pagesAmb 336 Case Study Analysisapi-336568710No ratings yet
- Examiners' Report June 2017: GCE Economics A 9EC0 03Document62 pagesExaminers' Report June 2017: GCE Economics A 9EC0 03nanami janinaNo ratings yet
- Exchange RatesDocument11 pagesExchange RatesElizavetaNo ratings yet
- Company accounts underwriting shares debenturesDocument7 pagesCompany accounts underwriting shares debenturesSakshi chauhanNo ratings yet
- Reference BikashDocument15 pagesReference Bikashroman0% (1)
- What Does Fedex Deliver?Document17 pagesWhat Does Fedex Deliver?duckythiefNo ratings yet
- Determination of Income, Consumption, SavingsDocument24 pagesDetermination of Income, Consumption, SavingsAmit PrabhakarNo ratings yet
- GEAR PPT Template OverviewDocument14 pagesGEAR PPT Template OverviewAmor MansouriNo ratings yet
- BlackBuck Looks To Disrupt B2B Logistics Market Apart From The Regular GPS-Enabled Freight Management, It Offers Features Such As Track and Trace, Truck Mapping - The Financial ExpressDocument2 pagesBlackBuck Looks To Disrupt B2B Logistics Market Apart From The Regular GPS-Enabled Freight Management, It Offers Features Such As Track and Trace, Truck Mapping - The Financial ExpressPrashant100% (1)
- QR 0298 Economy 17A 22:10: Boarding PassDocument2 pagesQR 0298 Economy 17A 22:10: Boarding PassannaNo ratings yet
- Sipcot 1Document1 pageSipcot 1sfdsddsNo ratings yet
- Barclays Capital - The - W - Ides of MarchDocument59 pagesBarclays Capital - The - W - Ides of MarchjonnathannNo ratings yet
- The Communistic Societies of The United StatesFrom Personal Visit and Observation by Nordhoff, Charles, 1830-1901Document263 pagesThe Communistic Societies of The United StatesFrom Personal Visit and Observation by Nordhoff, Charles, 1830-1901Gutenberg.org100% (2)
- SEMINAR KERJA PRAKTIK EVALUATES CDU FURNACESDocument41 pagesSEMINAR KERJA PRAKTIK EVALUATES CDU FURNACESMuhammad AswanNo ratings yet
- Original PDF Global Problems and The Culture of Capitalism Books A La Carte 7th EditionDocument61 pagesOriginal PDF Global Problems and The Culture of Capitalism Books A La Carte 7th Editioncarla.campbell348100% (41)