You might also like
- Valvular Heart DiseaseDocument2 pagesValvular Heart DiseaseAnonymous TVk12eX4No ratings yet
- Cardiac Stress TestingDocument24 pagesCardiac Stress TestingRhoda Dela Torre ContrerasNo ratings yet
- Valve SurgeriesDocument13 pagesValve SurgeriesShreeja SajitNo ratings yet
- Advanced Cardiac ProcedureDocument9 pagesAdvanced Cardiac ProcedureSachin DwivediNo ratings yet
- Cardiomyopathy: Leonard Shaju Joisy AloorDocument34 pagesCardiomyopathy: Leonard Shaju Joisy AloorJoisy AloorNo ratings yet
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNo ratings yet
- Cardiovascular and CVT Nursing TrendsDocument4 pagesCardiovascular and CVT Nursing TrendsShreyas Walvekar100% (1)
- Seminar On Shock: IntroductionDocument22 pagesSeminar On Shock: Introductionmahendra singhNo ratings yet
- Cardiac Enzyme StudiesDocument4 pagesCardiac Enzyme StudiesDara VinsonNo ratings yet
- Gastro Intestinal Bleeding DR - muayAD ABASSDocument59 pagesGastro Intestinal Bleeding DR - muayAD ABASSMAFADHELNo ratings yet
- Eric Berg CVDocument6 pagesEric Berg CVHaralambicNo ratings yet
- Hangnails and HomoeopathyDocument7 pagesHangnails and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Heart Muscle Shortness of Breath Tired Swelling of The Legs Heart Failure Irregular Heart Beat Fainting Sudden Cardiac DeathDocument6 pagesHeart Muscle Shortness of Breath Tired Swelling of The Legs Heart Failure Irregular Heart Beat Fainting Sudden Cardiac DeathSachin DwivediNo ratings yet
- Holter Monitor Guide for Heart Rhythm TrackingDocument19 pagesHolter Monitor Guide for Heart Rhythm TrackingRadison sierraNo ratings yet
- DefibrillationDocument9 pagesDefibrillationJara Maris Moreno BudionganNo ratings yet
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDocument9 pagesAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiNo ratings yet
- PERICARDITISDocument11 pagesPERICARDITISsalman hNo ratings yet
- Acute and Chronic Renal FailureDocument7 pagesAcute and Chronic Renal FailureSuliman GarallehNo ratings yet
- Cyanotic Congenital Heart DiseasesDocument25 pagesCyanotic Congenital Heart DiseasesAlvin OmondiNo ratings yet
- Hypertensive Heart DiseaseDocument33 pagesHypertensive Heart Diseaserini_adriani6817No ratings yet
- Aortic RegurgitationDocument19 pagesAortic RegurgitationsunilgenextNo ratings yet
- Demonstration On ParacentesisDocument10 pagesDemonstration On ParacentesisDeepika PrajapatiNo ratings yet
- Aortic StenosisDocument3 pagesAortic StenosisKhalid Mahmud Arifin100% (1)
- ECGDocument33 pagesECGTamia PutriNo ratings yet
- VSD Ventricular Septal Defect RepairDocument31 pagesVSD Ventricular Septal Defect RepairRedmond P. Burke MD100% (8)
- Holter Monitor: 'Ambulatory Electrocardiography Device''Document22 pagesHolter Monitor: 'Ambulatory Electrocardiography Device''Rachel PeredaNo ratings yet
- Arterial Line Arterial LineDocument13 pagesArterial Line Arterial LineLinamaria Lozano100% (1)
- Seminar On Rhuematic Heart DiseaseDocument16 pagesSeminar On Rhuematic Heart Diseasenaga maniNo ratings yet
- Valvular Heart DiseaseDocument54 pagesValvular Heart DiseaseRommanah AzmiNo ratings yet
- Cor PulmonaleDocument21 pagesCor Pulmonalemaibejose100% (1)
- Cardiac Tamponade and ManagementDocument42 pagesCardiac Tamponade and Managementأم حمدNo ratings yet
- Cardiogenic ShockDocument49 pagesCardiogenic Shockmaibejose0% (1)
- Cardiovascular System Diseases Part 2Document9 pagesCardiovascular System Diseases Part 2Prince Rener Velasco PeraNo ratings yet
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- Cardiomyopathy SeminarDocument17 pagesCardiomyopathy SeminarJyoti SinghNo ratings yet
- IntroductionDocument13 pagesIntroductionSiyara AntonyNo ratings yet
- Cataract BookDocument261 pagesCataract Bookstarsk777No ratings yet
- Cyanotic Heart DefectsDocument22 pagesCyanotic Heart DefectsCharlene ElioNo ratings yet
- Kano State College of Nursing and Midwifery: Cardiac ArrestDocument4 pagesKano State College of Nursing and Midwifery: Cardiac ArrestMuhammad Daha SanusiNo ratings yet
- Disorders of AortaDocument25 pagesDisorders of Aortavani reddyNo ratings yet
- ENT Nursing Care GuideDocument32 pagesENT Nursing Care GuideabdulNo ratings yet
- II.5. Pulmonary StenosisDocument12 pagesII.5. Pulmonary StenosisgenooehNo ratings yet
- PacemakersDocument19 pagesPacemakersAswathy RCNo ratings yet
- Treadmill Test: Khairul Nizam Abdul Rahman 4262143008Document12 pagesTreadmill Test: Khairul Nizam Abdul Rahman 4262143008Dea Amelia YolandaNo ratings yet
- Structure & Characterstics of Normal & Cancer CellsDocument58 pagesStructure & Characterstics of Normal & Cancer CellsVinay SahuNo ratings yet
- Assignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)Document7 pagesAssignment ON: TOPIC: PTCA (Percutaneous Transluminous Coronary Angioplasty)soniya josephNo ratings yet
- ArrhythmiasDocument48 pagesArrhythmiasHarshan JeyakumarNo ratings yet
- Ventricular Septal DefectsDocument7 pagesVentricular Septal DefectsMuhammadAldoGiansyahNo ratings yet
- Pulmonary EdemaaDocument17 pagesPulmonary EdemaaSoma Al-mutairiNo ratings yet
- CardioversionDocument48 pagesCardioversionDeeksha RajputNo ratings yet
- Heart BlockDocument20 pagesHeart BlockSumathi GopinathNo ratings yet
- Angioplasty.: Medical Surgical NursingDocument18 pagesAngioplasty.: Medical Surgical NursingAlma SusanNo ratings yet
- Radiation TherapyDocument2 pagesRadiation Therapyapi-446211408No ratings yet
- Mitral RegurgitationDocument9 pagesMitral RegurgitationNefvi Desqi AndrianiNo ratings yet
- Introduction Definition: Types of PacemakersDocument8 pagesIntroduction Definition: Types of PacemakersPrasann RoyNo ratings yet
- Ards PDFDocument2 pagesArds PDFgireeshsachinNo ratings yet
- Thrombolytic TherapyDocument16 pagesThrombolytic TherapyAnonymous nrZXFwNo ratings yet
- Mobile Coronary Care UnitDocument16 pagesMobile Coronary Care UnitArcha100% (2)
- Dr. Talha & Dr. Navya discuss abdominal trauma classification and managementDocument16 pagesDr. Talha & Dr. Navya discuss abdominal trauma classification and managementNavya BolluNo ratings yet
- Cardiac Arrest CPR GuideDocument54 pagesCardiac Arrest CPR GuideIdha FitriyaniNo ratings yet
- Child Ear Infection CausesDocument9 pagesChild Ear Infection CausesMona Santi NainggolanNo ratings yet
- B M W M: IO Edical Aste AnagementDocument23 pagesB M W M: IO Edical Aste AnagementJishnu JohnNo ratings yet
- Cardiac Cycle Events & PhasesDocument12 pagesCardiac Cycle Events & Phasesanupam manu100% (1)
- Causes, Symptoms and Nursing Care of AtherosclerosisDocument16 pagesCauses, Symptoms and Nursing Care of AtherosclerosisSAZZY ASHLEY GADDANGNo ratings yet
- Arrthyhmias: Conduction Blocks &Document126 pagesArrthyhmias: Conduction Blocks &Komal KhanodiaNo ratings yet
- Brady ArrhythmiasDocument36 pagesBrady ArrhythmiasSajin AlexanderNo ratings yet
- Electro Cardiogram & DysrythmiasDocument40 pagesElectro Cardiogram & DysrythmiasshobharamkrishnaNo ratings yet
- Heart BlockDocument30 pagesHeart BlockM Farhad KhaniNo ratings yet
- Abnormally High Proteins in Multiple MyelomaDocument23 pagesAbnormally High Proteins in Multiple MyelomamaibejoseNo ratings yet
- Dic - MNJDocument36 pagesDic - MNJmaibejoseNo ratings yet
- Wound HealingDocument23 pagesWound HealingmaibejoseNo ratings yet
- Valve Repair & ReplacementDocument27 pagesValve Repair & ReplacementmaibejoseNo ratings yet
- Health Declaration Form For ApplicantsDocument1 pageHealth Declaration Form For Applicantsgopeng glamping park malaysiaNo ratings yet
- Nursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDocument5 pagesNursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDr-Marudhar MarudharNo ratings yet
- Jomi 7657Document27 pagesJomi 7657casto.carpetasmiaNo ratings yet
- Anticestodal Drugs for Tapeworm TreatmentDocument3 pagesAnticestodal Drugs for Tapeworm TreatmentAbiHa YousaufNo ratings yet
- Autism and Dietary Therapy: Case Report and Review of The LiteratureDocument6 pagesAutism and Dietary Therapy: Case Report and Review of The LiteratureAntiopi PanteliNo ratings yet
- Congestive Heart Failure, Pulmonary Edema, and CPAPDocument35 pagesCongestive Heart Failure, Pulmonary Edema, and CPAPSherwan R Shal100% (1)
- ImmunosuppresentsDocument13 pagesImmunosuppresentsmadeputraNo ratings yet
- Health Check Template FormDocument2 pagesHealth Check Template Form백만호No ratings yet
- Stanford Letter Criticizes Trump COVID-19 AppointeeDocument11 pagesStanford Letter Criticizes Trump COVID-19 AppointeeBayAreaNewsGroup100% (2)
- English Nursing: Have You Gave A Chamber Pot To Mrs. Johnson?Document2 pagesEnglish Nursing: Have You Gave A Chamber Pot To Mrs. Johnson?Faris Albert WenasNo ratings yet
- Windkessel EffectDocument11 pagesWindkessel EffectAkhmad HidayatNo ratings yet
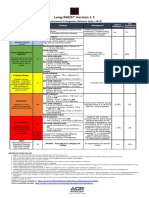
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Kasus Farter 2 10 Mei 2019Document3 pagesKasus Farter 2 10 Mei 2019YonicaryanNo ratings yet
- Effect of Temperature On FrogDocument2 pagesEffect of Temperature On FrogPrerna DubeyNo ratings yet
- Week 29 - DRRRDocument5 pagesWeek 29 - DRRRMira VeranoNo ratings yet
- HematologyDocument100 pagesHematologyerzaraptorNo ratings yet
- Journal BalakrishnaDocument3 pagesJournal BalakrishnafandheanayaNo ratings yet
- Vermikompos and Gliocladium Effectiveness Against Fusarium WiltDocument8 pagesVermikompos and Gliocladium Effectiveness Against Fusarium WiltJioWongMenengNo ratings yet
- IV Drug ReactionsDocument19 pagesIV Drug Reactionsphp_czarina04421No ratings yet
- Brain Death PPT VinayakDocument31 pagesBrain Death PPT Vinayakdrvinayakkodur100% (2)
- A Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostDocument6 pagesA Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostIJRASETPublicationsNo ratings yet
- QuestionsDocument6 pagesQuestionsLorvic Andrew Juanson UmaliNo ratings yet
- Diet PlanDocument6 pagesDiet Plantrical27 tricalNo ratings yet
- Triage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDDocument6 pagesTriage and Approach To The Acute Abdomen: Elisa M. Mazzaferro, MS, DVM, PHDRatna SariNo ratings yet
- Oral Health During Pregnancy - An Analysis of Information CoDocument8 pagesOral Health During Pregnancy - An Analysis of Information CoElena IancuNo ratings yet