You might also like
- Risk Assessment - Window and Glass Partition InstallationDocument4 pagesRisk Assessment - Window and Glass Partition Installationburak80% (5)
- Musculoskeletal 20,000 Series CPT Questions With Answers-CpcDocument16 pagesMusculoskeletal 20,000 Series CPT Questions With Answers-Cpcanchalnigam25100% (7)
- Omsite 2004 PDFDocument196 pagesOmsite 2004 PDFJulieNo ratings yet
- Miami Youth Football League Registration FormDocument1 pageMiami Youth Football League Registration FormMarley-Kojak CookNo ratings yet
- BSA Medical Form 680-001 A, B, C - 2014 PrintingDocument4 pagesBSA Medical Form 680-001 A, B, C - 2014 PrintingSarah Lowery FernandezNo ratings yet
- KT Chaser Product ManualDocument47 pagesKT Chaser Product Manualzx7blurr6239No ratings yet
- Uefa B AssignmentDocument23 pagesUefa B AssignmentArnelaŠabanovićNo ratings yet
- TM 10-8400-201-23&p General Repair Procedures For Clothing Oct. 2014Document612 pagesTM 10-8400-201-23&p General Repair Procedures For Clothing Oct. 2014GLOCK35100% (1)
- Die Casting SafetyDocument47 pagesDie Casting SafetyTrang Anh Toàn0% (1)
- UNDERAGEDocument1 pageUNDERAGEAngelica VidaNo ratings yet
- 2011 - 4 Year Old Tball RegistrationDocument2 pages2011 - 4 Year Old Tball RegistrationalabastercityhNo ratings yet
- 2011 Spring Soccer Registration Form 1-28-11Document1 page2011 Spring Soccer Registration Form 1-28-11jmercier74No ratings yet
- Fall 2011 RecRegistrationFormDocument1 pageFall 2011 RecRegistrationFormnikkistoneNo ratings yet
- Medical Release FormDocument1 pageMedical Release Formkelschriver12No ratings yet
- 2009 SCYTFC Registration FormDocument1 page2009 SCYTFC Registration FormvcexpressNo ratings yet
- Greater Houston Area Chapter American Red Cross Youth Volunteer Application FormDocument6 pagesGreater Houston Area Chapter American Red Cross Youth Volunteer Application FormLauren KhooNo ratings yet
- Registration Waiver-Release-Consent Form Clinics-CampsDocument1 pageRegistration Waiver-Release-Consent Form Clinics-Campsapi-101009897No ratings yet
- ESPIRIT de CORPS - Badminton Consent FormDocument2 pagesESPIRIT de CORPS - Badminton Consent Formrabi urangNo ratings yet
- Camp Jeff Waiver Form - 2021Document2 pagesCamp Jeff Waiver Form - 2021Nolan HahnNo ratings yet
- WAIVERDocument1 pageWAIVERlancemaala3No ratings yet
- RYBS 2016 RegistrationDocument2 pagesRYBS 2016 RegistrationKate SigurdsonNo ratings yet
- 2018 Bradford Fall Baseball RegistrationDocument1 page2018 Bradford Fall Baseball RegistrationAnthony LamaNo ratings yet
- Pre-K & Kindergarten Registration FormDocument1 pagePre-K & Kindergarten Registration FormEmily BowlesNo ratings yet
- Release FormDocument1 pageRelease Form3jarrettNo ratings yet
- Registration FormDocument1 pageRegistration FormccollettNo ratings yet
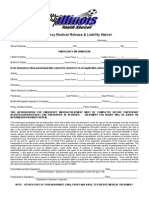
- Missouri Emergency Medical Release FormDocument1 pageMissouri Emergency Medical Release FormitargetingNo ratings yet
- MedicalreleaseDocument1 pageMedicalreleaseapi-262949858No ratings yet
- Key-Club-Membership-Form 1Document4 pagesKey-Club-Membership-Form 1api-461627977No ratings yet
- JR High 2010 Registration FormDocument4 pagesJR High 2010 Registration FormryanlashleeNo ratings yet
- Consent Don PepotDocument1 pageConsent Don PepotJERUSALEM DE GUZMANNo ratings yet
- 2011 Spring SOCCER Registration FormDocument3 pages2011 Spring SOCCER Registration FormalabastercityhNo ratings yet
- Individual (Minor) Registration 2011 2012 2Document3 pagesIndividual (Minor) Registration 2011 2012 2Reka KovacsNo ratings yet
- Af Cavemen Cheer Try-Out PacketDocument5 pagesAf Cavemen Cheer Try-Out PacketAf CheerNo ratings yet
- 2019 April Vacation Horse Camp at Mack Hill Riding AcademyDocument4 pages2019 April Vacation Horse Camp at Mack Hill Riding AcademyLauren SmithNo ratings yet
- 2018 Bradford Fall Baseball RegistrationDocument1 page2018 Bradford Fall Baseball RegistrationAnthony LamaNo ratings yet
- YOUTH Student Info FormDocument1 pageYOUTH Student Info FormAnonymous 5jdRdlUZNo ratings yet
- Players AgreementDocument2 pagesPlayers Agreementapi-446343989No ratings yet
- Junior Patriot Basketball League BOYS SIGNUPS: Grades 2 Through 4Document4 pagesJunior Patriot Basketball League BOYS SIGNUPS: Grades 2 Through 4api-217089716No ratings yet
- Go BIG For Parkinson Registration FormDocument2 pagesGo BIG For Parkinson Registration Formrickberry55No ratings yet
- 1st Through 6th Registration FormDocument1 page1st Through 6th Registration FormEmily BowlesNo ratings yet
- 2013-2014 Returning Medical FormDocument10 pages2013-2014 Returning Medical FormKevin WangNo ratings yet
- Velocity Health FormDocument2 pagesVelocity Health FormChris HansenNo ratings yet
- WaiverDocument1 pageWaiverMel PubgmNo ratings yet
- Batang Pinoy Waiver and Release From LiabilityDocument1 pageBatang Pinoy Waiver and Release From LiabilityImelda QuintosNo ratings yet
- Registration Form May 23Document9 pagesRegistration Form May 23Krishn PatelNo ratings yet
- Contest WaiverDocument1 pageContest Waiverapi-252347024No ratings yet
- Edmonton Columbians Track & Field Club: Athlete - Coach - Volunteer - OtherDocument4 pagesEdmonton Columbians Track & Field Club: Athlete - Coach - Volunteer - Otherget_phat_nowNo ratings yet
- Consent and Release From Liability Certificate: Florida High School Athletic AssociationDocument5 pagesConsent and Release From Liability Certificate: Florida High School Athletic AssociationandrewNo ratings yet
- Gig Harbor Volleyball Club ReleaseDocument1 pageGig Harbor Volleyball Club Releasehonni_33No ratings yet
- Fillable INTERNATIONAL VOLLEYBALL WAIVER PDFDocument3 pagesFillable INTERNATIONAL VOLLEYBALL WAIVER PDFMcKensie HeroldNo ratings yet
- SV GLORY Medical Release-Emergency Form & Liability Waiver FormDocument2 pagesSV GLORY Medical Release-Emergency Form & Liability Waiver FormfcuevasNo ratings yet
- Accepted. Please Send The Completed Forms ToDocument18 pagesAccepted. Please Send The Completed Forms ToAmber Schmidt DoopNo ratings yet
- Inter College Team Sports Basketball Volleyball MechanicsDocument2 pagesInter College Team Sports Basketball Volleyball MechanicsZhennaica Coreen NavarroNo ratings yet
- Medical Release FormDocument1 pageMedical Release FormNicole LeongNo ratings yet
- Baseball Camp 18 1Document1 pageBaseball Camp 18 1api-267310659No ratings yet
- 2018 April Vacation Tournament at Mack Hill Riding AcademyDocument4 pages2018 April Vacation Tournament at Mack Hill Riding AcademyLauren SmithNo ratings yet
- Field Trip Permission Slip FillableDocument1 pageField Trip Permission Slip Fillabletvtcf286v9No ratings yet
- HG WaiverDocument1 pageHG WaiverOrlando DiazNo ratings yet
- Santa 2010 Shiai Reg Ver5Document2 pagesSanta 2010 Shiai Reg Ver5BananatearerNo ratings yet
- Philippine National Games 2023: Parental Consent, Waiver & ReleaseDocument1 pagePhilippine National Games 2023: Parental Consent, Waiver & ReleaseAntonio Ponce Valenzuela Jr.No ratings yet
- PNGSL Player Registration Form: Parents' InformationDocument1 pagePNGSL Player Registration Form: Parents' InformationMonique BatsonNo ratings yet
- HG WaiverDocument1 pageHG WaiverOrlando DiazNo ratings yet
- SummersportsDocument1 pageSummersportsapi-318790212No ratings yet
- 2019 Chicago Marathon Waiver and Commitment Form - Guaranteed ExDocument3 pages2019 Chicago Marathon Waiver and Commitment Form - Guaranteed ExSeanSean ParkNo ratings yet
- Surprise Youth Soccer Liability ReleaseDocument1 pageSurprise Youth Soccer Liability ReleaseGilbert AngelNo ratings yet
- 09 Lec NotesDocument9 pages09 Lec NotesEvilasio CostaNo ratings yet
- 2015 FIAT 500 Abarth Owners ManualDocument428 pages2015 FIAT 500 Abarth Owners ManualFiat500USANo ratings yet
- Chicken Lab Formal ReportDocument5 pagesChicken Lab Formal Reportapi-378518499No ratings yet
- Version FinalDocument22 pagesVersion FinalsanthiyasandyNo ratings yet
- Anatomy I MCQ PDFDocument2 pagesAnatomy I MCQ PDFBilal AhmadNo ratings yet
- Australian - 2008 - Maxillofacial Trauma in Major Trauma PatientsDocument6 pagesAustralian - 2008 - Maxillofacial Trauma in Major Trauma Patientsووويويويةءتؤوبةين للاNo ratings yet
- Wrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHDocument22 pagesWrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHMd Ahsanuzzaman PinkuNo ratings yet
- Hearing Loss - A Clinical ApproachDocument70 pagesHearing Loss - A Clinical ApproachJohnson Jayaraj100% (2)
- St. Mary's Academy Case DigestDocument4 pagesSt. Mary's Academy Case DigestMicaela Dela PeñaNo ratings yet
- Bolted Connection FatigueDocument12 pagesBolted Connection FatigueMahfuzur Rahman100% (1)
- First Aid:: Head and Spine InjuryDocument14 pagesFirst Aid:: Head and Spine InjuryJulia FlorencioNo ratings yet
- Horno kd250Document48 pagesHorno kd250Steeve FigueroaNo ratings yet
- Eathe.2016.1080p.webrip.x264.aac2.0 StuttershitDocument38 pagesEathe.2016.1080p.webrip.x264.aac2.0 StuttershitUmaNo ratings yet
- Parotidectomy: H.Shameer AhamedDocument47 pagesParotidectomy: H.Shameer AhamedAndreas RendraNo ratings yet
- Simple Past, Past Progressive, Past Perfect Simple, Past Perfect ProgressiveDocument3 pagesSimple Past, Past Progressive, Past Perfect Simple, Past Perfect ProgressiveDiana LuncasuNo ratings yet
- Parade 2 Februari 2023 Tanpa AsaDocument25 pagesParade 2 Februari 2023 Tanpa Asaputra syawalNo ratings yet
- Encounters in The UnderdarkDocument4 pagesEncounters in The UnderdarkRafael FrançaNo ratings yet
- Wallflowers Wish - A Marquess For Miss MarigoldDocument144 pagesWallflowers Wish - A Marquess For Miss MarigoldFlia Garcia33% (3)
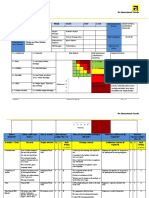
- Risk AssessmentDocument2 pagesRisk Assessmentsonia_rachNo ratings yet
- Gadar 220190401Document7 pagesGadar 220190401muhammad pratamaNo ratings yet
- Carpal Tunnel SyndromeDocument24 pagesCarpal Tunnel SyndromeReymond GuevarraNo ratings yet
- Plex Nonskeletal Problems in Preadolescent ChildrenDocument5 pagesPlex Nonskeletal Problems in Preadolescent ChildrenyasmineNo ratings yet
- What Are The Benefits of Chiropractic CareDocument2 pagesWhat Are The Benefits of Chiropractic CaretomNo ratings yet