You might also like
- The Effectiveness of Galactomyces FermentDocument6 pagesThe Effectiveness of Galactomyces FermentFransiscus Clinton100% (1)
- Lect 3 Trauma CounsellingDocument28 pagesLect 3 Trauma Counsellingumibrahim75% (8)
- Naskah Publikasi LansiaDocument17 pagesNaskah Publikasi LansiaVhiny ChaNo ratings yet
- Hubungan Imt Dengan RADocument5 pagesHubungan Imt Dengan RAlindapramusintaNo ratings yet
- Daftar Pustaka StuntingDocument1 pageDaftar Pustaka StuntingtomoandiNo ratings yet
- Penyakit Menular SeksualDocument100 pagesPenyakit Menular Seksualkaterinindah100% (1)
- Advance Care Planning English VersionDocument9 pagesAdvance Care Planning English VersionAlma NurfitriaNo ratings yet
- Jurnal Aulia Abidzah, S.K.M PDFDocument10 pagesJurnal Aulia Abidzah, S.K.M PDFJamilah Sinaga100% (1)
- Systemic Lupus Erythematosus (SLE) : Pembimbing: Dr. Sondang M Lumban Batu, Sp.ADocument36 pagesSystemic Lupus Erythematosus (SLE) : Pembimbing: Dr. Sondang M Lumban Batu, Sp.AWinda Oktavia PakpahanNo ratings yet
- Jurnal Hepatitis BDocument42 pagesJurnal Hepatitis BGiffari AnugrahNo ratings yet
- Clinical Practice Guidelines For The Management of DepressionDocument17 pagesClinical Practice Guidelines For The Management of DepressionAnamika SinhaNo ratings yet
- Hubungan Antara Tingkat Pengetahuan Dan Sikap Ibu Dalam Pencegahan Ispa Dengan Kejadian Ispa Pada Anak Balita Di Desa Pucangan Wilayah Kerja Puskesmas Kartasura IDocument9 pagesHubungan Antara Tingkat Pengetahuan Dan Sikap Ibu Dalam Pencegahan Ispa Dengan Kejadian Ispa Pada Anak Balita Di Desa Pucangan Wilayah Kerja Puskesmas Kartasura IReza Syahbandi Jasma Wijaya100% (2)
- Diagnosis Dan Diagnosis Banding DM SK 2Document99 pagesDiagnosis Dan Diagnosis Banding DM SK 2syahron maskatNo ratings yet
- Bhasa InggrisDocument23 pagesBhasa InggrisrinaNo ratings yet
- Standar Operasional Prosedur (Sop) Teknik Relaksasi Nafas DalamDocument1 pageStandar Operasional Prosedur (Sop) Teknik Relaksasi Nafas DalamNERS ANGKATAN 8No ratings yet
- Mobilisasi Dan Fisioterapi-Vap PDFDocument9 pagesMobilisasi Dan Fisioterapi-Vap PDFYANNo ratings yet
- Indonesia Maternal Health Articles - Abstracts - NeonatalDocument92 pagesIndonesia Maternal Health Articles - Abstracts - Neonatalnova seftya aristadilaNo ratings yet
- Siska Tri Silviani - 0432950318051 - Analisa Jurnal Terapi Konvensional Dan Komplementer Kelompok 8Document9 pagesSiska Tri Silviani - 0432950318051 - Analisa Jurnal Terapi Konvensional Dan Komplementer Kelompok 8Siska Tri SilvianiNo ratings yet
- Paper About Covid-19 Virus: D I S U S U N OlehDocument10 pagesPaper About Covid-19 Virus: D I S U S U N OlehRia Waruwu100% (1)
- Obes 2 PDFDocument10 pagesObes 2 PDFNabilla YuharlinaNo ratings yet
- Pengaruh Pemberian Bawang Putih Terhadappenurunan Kadar Kolesterol Pada Lansia Wilayah Kerja PuskesmasdelituaDocument10 pagesPengaruh Pemberian Bawang Putih Terhadappenurunan Kadar Kolesterol Pada Lansia Wilayah Kerja PuskesmasdelituaAttila JonesNo ratings yet
- ID Faktor Faktor Yang Mempengaruhi PerilakuDocument11 pagesID Faktor Faktor Yang Mempengaruhi PerilakuM Ekmal Yusuf PutraNo ratings yet
- Jurnal SIK Pengembangan SIKNAS Di Lampung 2018Document16 pagesJurnal SIK Pengembangan SIKNAS Di Lampung 2018ELLIYAWATINo ratings yet
- Athens Insomnia Scale QuestionnaireDocument2 pagesAthens Insomnia Scale QuestionnaireakuerwinNo ratings yet
- Laporan B1 Mar 2018Document2 pagesLaporan B1 Mar 2018puskesmas situ gintungNo ratings yet
- TB Paru FK UncenDocument66 pagesTB Paru FK UncenAndira Trianingrum TukanNo ratings yet
- Congenital AnomaliDocument59 pagesCongenital AnomaliFaqih Bawazir SNo ratings yet
- Dosen Pembimbing Jeni Cesi Cintiani, SSTDocument1 pageDosen Pembimbing Jeni Cesi Cintiani, SSTitaNo ratings yet
- Aqcuired Immunodeficiency SyndromeDocument78 pagesAqcuired Immunodeficiency SyndromeandiariansyahNo ratings yet
- Eliza Halim PDFDocument209 pagesEliza Halim PDFirma arivitaNo ratings yet
- Travel MedicineDocument63 pagesTravel MedicineINdri Nur SutantiNo ratings yet
- Memahami Prima FacieDocument26 pagesMemahami Prima Faciewicak_spNo ratings yet
- Artikel Kesehatan Bahasa Inggris: Keeping Skin Healthy and Beautiful, Do Not Need Expensive!Document2 pagesArtikel Kesehatan Bahasa Inggris: Keeping Skin Healthy and Beautiful, Do Not Need Expensive!Anonymous IKgbeVoNo ratings yet
- Perbedaan Efektifitas Madu Dan Air Gula Terhadap Nyeri Injeksi Imunisasi Campak Bayi Usia 9-15 Bulan Puskesmas Lubuk Buaya TAHUN 2019Document12 pagesPerbedaan Efektifitas Madu Dan Air Gula Terhadap Nyeri Injeksi Imunisasi Campak Bayi Usia 9-15 Bulan Puskesmas Lubuk Buaya TAHUN 2019Herlin YofitasariNo ratings yet
- Register Poli Umum Februari 2023Document127 pagesRegister Poli Umum Februari 2023Nita YatoNo ratings yet
- Anemia Pada KehamilanDocument27 pagesAnemia Pada KehamilanWidya AsmiNo ratings yet
- Hubungan Stres Dengan Kualitas Hidup Penderita Diabetes Mellitus Tipe 2Document9 pagesHubungan Stres Dengan Kualitas Hidup Penderita Diabetes Mellitus Tipe 2Wirda RinaNo ratings yet
- Combustio Grade II A + BDocument16 pagesCombustio Grade II A + BDyna Eka AlphattinsonNo ratings yet
- BMI-U Persentil (2-20) BoysDocument1 pageBMI-U Persentil (2-20) BoysHeri Hrisikesa WjgNo ratings yet
- Kaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraDocument2 pagesKaplan, Sadock, Grebb. 1997. Sinopsis Psikiatri Ilmu Pengetahuan Perilaku Psikiatri Klinis Jilid Satu. Jakarta: Binarupa AksaraLordeNo ratings yet
- Pengaruh Kebiasaan Merokok Keluarga Di Dalam Rumah: AbstrakDocument23 pagesPengaruh Kebiasaan Merokok Keluarga Di Dalam Rumah: Abstraknisa mustikaNo ratings yet
- Jurnal RubellaDocument2 pagesJurnal RubellaAlif SpiritNo ratings yet
- Eka Aryani 22010112110093 Lap KTI BAB 7Document36 pagesEka Aryani 22010112110093 Lap KTI BAB 7Aldis Al FadjrinNo ratings yet
- Kebijakan Kesehatan Ibu Dan Anak Di IndonesiaDocument24 pagesKebijakan Kesehatan Ibu Dan Anak Di IndonesiaSurahmanAhmadNo ratings yet
- SGD 11 - Zayyina Chamaladina - 30101900210Document8 pagesSGD 11 - Zayyina Chamaladina - 30101900210Anonymous iTstegX2No ratings yet
- Seminar ISTC TB Feb 2016Document12 pagesSeminar ISTC TB Feb 2016christine nathalia loupattyNo ratings yet
- Overview of The Mucopolysaccharidoses: RheumatologyDocument9 pagesOverview of The Mucopolysaccharidoses: RheumatologyLaura Orjuela MateusNo ratings yet
- Slide Bonviva 1Document34 pagesSlide Bonviva 1Maksum PandelimaNo ratings yet
- Hiv AidsDocument59 pagesHiv Aidsnadifa nadaNo ratings yet
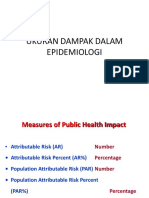
- UKURAN DAMPAK DALAM EPIDEMIOLOGI KelompokDocument24 pagesUKURAN DAMPAK DALAM EPIDEMIOLOGI KelompokcindyNo ratings yet
- Case ReportDocument47 pagesCase ReportAriefNo ratings yet
- OsteoarthritisDocument61 pagesOsteoarthritisTony HermawanNo ratings yet
- Data - anggotaKABUPATEN SIJUNJUNG-1Document8 pagesData - anggotaKABUPATEN SIJUNJUNG-1deviya srimarlisNo ratings yet
- Pharmacogenomics: From Discovery to Clinical ImplementationFrom EverandPharmacogenomics: From Discovery to Clinical ImplementationShowkat Ahmad GanieNo ratings yet
- Bagian Perinatologi: Informasi Lebih Lanjut Silahkan HubungiDocument2 pagesBagian Perinatologi: Informasi Lebih Lanjut Silahkan HubungigodeNo ratings yet
- Retinopati DiabetikDocument5 pagesRetinopati DiabetikMuhammad Afriadi HamdanNo ratings yet
- Kuliah - Obesity - Metabolic Syndrome 2012Document45 pagesKuliah - Obesity - Metabolic Syndrome 2012Harrison BungasaluNo ratings yet
- Pengkajian Pasien GeriatriDocument24 pagesPengkajian Pasien GeriatriLoudry ElfaNo ratings yet
- Skin and Soft Tissue Infection InfoDocument4 pagesSkin and Soft Tissue Infection InfoPresura Andreea IulianaNo ratings yet
- Infeksi StreptoDocument6 pagesInfeksi StreptoRiris SutrisnoNo ratings yet
- Necrotizing Soft Tissue Infections: A Primary Care ReviewDocument6 pagesNecrotizing Soft Tissue Infections: A Primary Care ReviewYeni PuspitasariNo ratings yet
- Andersen Mcfarlane Wheel-1 2Document17 pagesAndersen Mcfarlane Wheel-1 2api-532703094No ratings yet
- Bed Bathing A PatientDocument5 pagesBed Bathing A PatientsalmaisazbouredNo ratings yet
- Sequalae of Wearing Complete DenturesDocument34 pagesSequalae of Wearing Complete DenturesAyeshaAslamNo ratings yet
- OHS-PR-09-03-F02 RISK ASSESSMENT For INSTALLATION OF WALL MOUNTED JIB CRANEDocument21 pagesOHS-PR-09-03-F02 RISK ASSESSMENT For INSTALLATION OF WALL MOUNTED JIB CRANEmohammed tofiqNo ratings yet
- Bioethics MidtermDocument51 pagesBioethics MidtermHello TalkNo ratings yet
- Top Muscle Building and Weight Gain SecretsDocument8 pagesTop Muscle Building and Weight Gain SecretsKarl Gallagher83% (6)
- NCP CopdDocument4 pagesNCP CopdJoshua ValdrizNo ratings yet
- How To Survive Family LifeDocument16 pagesHow To Survive Family LiferoberttNo ratings yet
- TwinkyStar BrosuraDocument4 pagesTwinkyStar BrosuraFlorin Cornel VelcuNo ratings yet
- Weight Percentiles CalculatorDocument1 pageWeight Percentiles CalculatorSubhan Arif RahmanNo ratings yet
- R08 HE3C32 TIE PLN HS 0004 Emergency Response PlanDocument27 pagesR08 HE3C32 TIE PLN HS 0004 Emergency Response PlanHafiz ZameerNo ratings yet
- Disorders of Blood Pressure Regulation - 10Document31 pagesDisorders of Blood Pressure Regulation - 10Cres Padua QuinzonNo ratings yet
- Park SoftDocument942 pagesPark Softnaresh chauhanNo ratings yet
- How To Read A CTG: What Is Cardiotocography?Document11 pagesHow To Read A CTG: What Is Cardiotocography?Rinothja RajaratnamNo ratings yet
- Jurnal HiperbilirubinemiaDocument5 pagesJurnal HiperbilirubinemiaWahyumi AmboahaNo ratings yet
- EWC 661 English For Report Writing: Prepared By: NO Name Student IdDocument7 pagesEWC 661 English For Report Writing: Prepared By: NO Name Student IdAthirah Dinata100% (1)
- PT 1 Midterm RubricDocument3 pagesPT 1 Midterm RubricJohann Sebastian CruzNo ratings yet
- Assignment On-: "Pharmacokinetics of Drug Molecules in Different Disease Condition"Document19 pagesAssignment On-: "Pharmacokinetics of Drug Molecules in Different Disease Condition"Susmoy SinhaNo ratings yet
- Acute Gastroenteritis REPORTDocument11 pagesAcute Gastroenteritis REPORTMelai Barneso Leal100% (1)
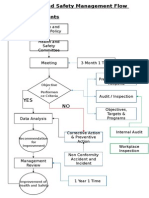
- Health and Safety FlowDocument6 pagesHealth and Safety Flowzaki0304No ratings yet
- Vasculitis When To Consider This DiagnosisDocument15 pagesVasculitis When To Consider This DiagnosisAndres PortesNo ratings yet
- Ranjit Kumar-Research Methodology A Step-by-Step G-25-26Document2 pagesRanjit Kumar-Research Methodology A Step-by-Step G-25-26Trendy NewsNo ratings yet
- RRL On HospitalsDocument13 pagesRRL On HospitalsNellyn GutierrezNo ratings yet
- 50 Item Integumentary Exam-BudekDocument8 pages50 Item Integumentary Exam-BudekLj FerolinoNo ratings yet
- Clinical Applied Anatomy in Wound CareDocument18 pagesClinical Applied Anatomy in Wound CareKlinik Komuniti Perwira100% (2)
- NCM109Document4 pagesNCM109Cherry Ann Cagayat MadrigalNo ratings yet
- NBHS 1104 Topic 2Document18 pagesNBHS 1104 Topic 2hema angleNo ratings yet
- KodefDocument45 pagesKodefWann FarhannaNo ratings yet
- Acidemia and HyperkalemiaDocument1 pageAcidemia and HyperkalemiaDennis Nabor Muñoz, RN,RMNo ratings yet