You might also like
- Cleft Lip and Palate Management: A Comprehensive AtlasFrom EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunNo ratings yet
- Atlas of Topographical and Pathotopographical Anatomy of the Head and NeckFrom EverandAtlas of Topographical and Pathotopographical Anatomy of the Head and NeckNo ratings yet
- Surgical Anatomy of Mandible DeptDocument92 pagesSurgical Anatomy of Mandible Deptbhavaaishu100% (1)
- Development of MandibleDocument60 pagesDevelopment of MandibleAlisha Aranha100% (1)
- Growth and Development of Mandible KiranDocument92 pagesGrowth and Development of Mandible Kirannavjotsinghjassal100% (1)
- Prenatal & Postnatal Growth of MandibleDocument44 pagesPrenatal & Postnatal Growth of MandibleAnkur SharmaNo ratings yet
- Development of Face and AnomaliesDocument69 pagesDevelopment of Face and AnomaliesgoksdentNo ratings yet
- Development of The Mandible: Dr. Kemer KDocument41 pagesDevelopment of The Mandible: Dr. Kemer KLintoNo ratings yet
- MandibleDocument120 pagesMandibleArnab SantraNo ratings yet
- Applied Anatomy of Maxilla and Mandible RepeatDocument143 pagesApplied Anatomy of Maxilla and Mandible RepeatNamshi Ahamed100% (3)
- Anatomy and Physiology of Temporomandibular JointDocument12 pagesAnatomy and Physiology of Temporomandibular JointSharlene OngNo ratings yet
- Alveolar Bone GraftingDocument38 pagesAlveolar Bone GraftingMohammed Qasim Al-Watary100% (1)
- Alveolar Bone DR DeepakDocument107 pagesAlveolar Bone DR DeepakDeepak Kumar100% (2)
- Mandibular MovementsDocument36 pagesMandibular MovementsRagini ShravanNo ratings yet
- Muscles of MasticationDocument50 pagesMuscles of MasticationKaran AroraNo ratings yet
- Trigeminal Nerve Seminar FINALDocument54 pagesTrigeminal Nerve Seminar FINALAnji Satsangi100% (1)
- Submandibular Gland AnatomyDocument26 pagesSubmandibular Gland AnatomysupritiNo ratings yet
- 8 Surgical Anatomy of TMJDocument11 pages8 Surgical Anatomy of TMJArchanaShenoyNo ratings yet
- Development of Tooth Lecture-1Document63 pagesDevelopment of Tooth Lecture-1Dimple KashyapNo ratings yet
- Extraoral and Intraoral ExaminationDocument64 pagesExtraoral and Intraoral ExaminationAhmed HotiebaNo ratings yet
- Enamel: Click To Edit Master Subtitle StyleDocument106 pagesEnamel: Click To Edit Master Subtitle StyleManva MonishNo ratings yet
- Local Anesthesia Techniques in Oral and Maxillofacial SurgeryDocument102 pagesLocal Anesthesia Techniques in Oral and Maxillofacial Surgerydr_jamal1983No ratings yet
- Post Natal Development of MandibleDocument45 pagesPost Natal Development of MandibleSamarth VajpayeeNo ratings yet
- Growth & Dev - of MaxillaDocument26 pagesGrowth & Dev - of Maxillaharshita parasharNo ratings yet
- Flaps in Maxillofacial ReconstructionDocument29 pagesFlaps in Maxillofacial ReconstructionJaspreet Kaur33% (3)
- Maxillary ObturatorDocument79 pagesMaxillary ObturatorAmit KhattakNo ratings yet
- Ellis FracturesDocument40 pagesEllis Fracturespriti adsulNo ratings yet
- CEMENTUMDocument50 pagesCEMENTUMDENTALORG.COM100% (1)
- Mandibular Anatomical LandmarksDocument14 pagesMandibular Anatomical LandmarksKishor Chindam100% (4)
- Zygomatic Arch and Orbital FracturesDocument6 pagesZygomatic Arch and Orbital FractureszacrouchyNo ratings yet
- Dental Anatomy Final ReviewDocument10 pagesDental Anatomy Final ReviewSalma AhmedNo ratings yet
- Growth and Development Maxilla and MandibleDocument42 pagesGrowth and Development Maxilla and MandibleDrMudit Kumar100% (4)
- Development of Palate and Tongue NotesDocument9 pagesDevelopment of Palate and Tongue NotesClarisse MendozaNo ratings yet
- 002.pre-Natal & Post-Natal Growth & Development of MaxillaDocument153 pages002.pre-Natal & Post-Natal Growth & Development of Maxillapriti adsul100% (1)
- The MandibleDocument115 pagesThe MandiblenavjotsinghjassalNo ratings yet
- Difference Between Primary Permanent Dentition PedoDocument17 pagesDifference Between Primary Permanent Dentition PedoFourthMolar.comNo ratings yet
- Developmentofteeth StagesDocument45 pagesDevelopmentofteeth Stagesimi4100% (1)
- 300 Dental Anatomy Facts - NBDEDocument13 pages300 Dental Anatomy Facts - NBDEmilagros falconNo ratings yet
- Methods of Space Gaining in OrthodonticsDocument41 pagesMethods of Space Gaining in OrthodonticsAwas AwasNo ratings yet
- Osteology of MandibleDocument40 pagesOsteology of MandibleYamini RampriyaNo ratings yet
- Mandibular Second PremolarDocument13 pagesMandibular Second Premolarxmarty.fazilNo ratings yet
- OMFS Clinics Exam Notes V Course 2020Document330 pagesOMFS Clinics Exam Notes V Course 2020Vagelis RaftopoulosNo ratings yet
- Department of Pediatrics and Preventive Dentistry.: Local Anasthesia in Pediatric DentistryDocument27 pagesDepartment of Pediatrics and Preventive Dentistry.: Local Anasthesia in Pediatric DentistrySudip ChakrabortyNo ratings yet
- Growth and Development of Maxilla / Orthodontic Courses by Indian Dental AcademyDocument63 pagesGrowth and Development of Maxilla / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- 3rd Molar ImpactionDocument31 pages3rd Molar ImpactionPuneet Jain100% (1)
- 01 - 20131119 Skull IDocument56 pages01 - 20131119 Skull INancyLiao100% (2)
- On ImpactionDocument44 pagesOn Impactionmesssi269No ratings yet
- Development of OcclusionDocument119 pagesDevelopment of Occlusiondentistpro.org100% (7)
- Alveolar BoneDocument50 pagesAlveolar Boneanchal100% (1)
- Muscles of MasticationDocument23 pagesMuscles of Masticationبراءة أحمد السلامات100% (1)
- Oral HistologyDocument6 pagesOral HistologyMr. Orange100% (2)
- Periodontium (2) - Gingiva: Microscopic Features of GingivaDocument8 pagesPeriodontium (2) - Gingiva: Microscopic Features of Gingivaمحمد محمود القحيفNo ratings yet
- Definition:: Types of Forceps Used For Tooth ExtractionDocument28 pagesDefinition:: Types of Forceps Used For Tooth Extractionayman moaed alyasen100% (1)
- Temporomandibular DisordersDocument45 pagesTemporomandibular DisordersMohsin HabibNo ratings yet
- The Making of British Oral and Maxillofacial SurgeryFrom EverandThe Making of British Oral and Maxillofacial SurgeryRating: 4 out of 5 stars4/5 (1)
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideFrom EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideNo ratings yet
- Essential Tissue Healing of the Face and NeckFrom EverandEssential Tissue Healing of the Face and NeckRating: 5 out of 5 stars5/5 (2)
- September 2004 Paper2Document10 pagesSeptember 2004 Paper2api-26291651100% (2)
- Cranial Nerve AssessmentDocument17 pagesCranial Nerve AssessmentMahendran Jayaraman100% (1)
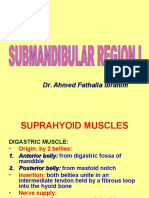
- 14-Submandibular Region IDocument21 pages14-Submandibular Region IvelangniNo ratings yet
- Golgi Tendon ReflexDocument15 pagesGolgi Tendon ReflexDemuel Dee L. BertoNo ratings yet
- Physiology of Digestive SystemDocument10 pagesPhysiology of Digestive SystemOm AbdalrahmanNo ratings yet
- Salivary Gland-Mind MapDocument3 pagesSalivary Gland-Mind Mapamaansyed2190No ratings yet
- ACP, ch2, 2.6.1 and 2.6.2, Khalid AlshareefDocument3 pagesACP, ch2, 2.6.1 and 2.6.2, Khalid AlshareefKhalid Bin FaisalNo ratings yet
- Physiology of Renal SystemDocument28 pagesPhysiology of Renal SystemKhalid AbdullahNo ratings yet
- Tetanic Contraction - WikipediaDocument9 pagesTetanic Contraction - WikipediaSIBANI CHAUDHURYNo ratings yet
- AnaPhy - Digestive SystemDocument5 pagesAnaPhy - Digestive SystemJan Mark SotoNo ratings yet
- Assessment of Breast and Lymphatic SystemDocument4 pagesAssessment of Breast and Lymphatic Systemclyde i amNo ratings yet
- Blood Transfusion NotesDocument1 pageBlood Transfusion NotesShreyas WalvekarNo ratings yet
- Abdominal X RayDocument45 pagesAbdominal X RayAbdullah As'adNo ratings yet
- Blood Vessels, AnatomyDocument20 pagesBlood Vessels, AnatomyAbu BakarNo ratings yet
- Breathing TechniquesDocument26 pagesBreathing TechniquessherryNo ratings yet
- Division of Catbalogan City Junior High School Semi-Detailed Lesson Plan in Science Learning CompetencyDocument4 pagesDivision of Catbalogan City Junior High School Semi-Detailed Lesson Plan in Science Learning Competencyjestony matillaNo ratings yet
- Understanding Autoimmune Disease PDFDocument18 pagesUnderstanding Autoimmune Disease PDFLiz TaylorNo ratings yet
- Insufisiensi Vena Kronik: Akina Maulidhany Tahir, M.DDocument12 pagesInsufisiensi Vena Kronik: Akina Maulidhany Tahir, M.Dummu yayaNo ratings yet
- Blood Components PDFDocument1 pageBlood Components PDFFATIN NAJIHAHNo ratings yet
- Animal Tissues 22Document8 pagesAnimal Tissues 22Arleen ColacionNo ratings yet
- Medical Terminology Cardiovascular SystemDocument35 pagesMedical Terminology Cardiovascular Systemapi-26819951486% (7)
- Surgery Oman MCQDocument49 pagesSurgery Oman MCQAsif NewazNo ratings yet
- Answers To End-Of-Chapter Questions Chapter 9: Transport in AnimalsDocument2 pagesAnswers To End-Of-Chapter Questions Chapter 9: Transport in AnimalsGabriele Caruso67% (3)
- Neuro Lab Physio Ex 6.0Document13 pagesNeuro Lab Physio Ex 6.0KevinDelaCruzNo ratings yet
- Full-Mouth Adhesive Rehabilitation of A Severely Eroded Dentition: The Three-Step Technique. Part 1Document95 pagesFull-Mouth Adhesive Rehabilitation of A Severely Eroded Dentition: The Three-Step Technique. Part 1RichbenavidesNo ratings yet
- The PharynxDocument67 pagesThe PharynxArvindhanNo ratings yet
- LE3219 - Leather Microbiology Infection and ImmunityDocument21 pagesLE3219 - Leather Microbiology Infection and ImmunityAnik AlamNo ratings yet
- Theories of Growth and DevelopmentDocument105 pagesTheories of Growth and DevelopmentAjmal Najeeb50% (2)
- Old Question Mbbs 200809Document9 pagesOld Question Mbbs 200809Manish SarkarNo ratings yet
- 10.4 Homeostasis-1Document10 pages10.4 Homeostasis-1صالح ابراهيمNo ratings yet