You might also like
- Certification of No Pending Case DimeDocument1 pageCertification of No Pending Case DimeGilbert Guzman Turaray100% (1)
- Minutes of The 42nd General Assembly PDFDocument17 pagesMinutes of The 42nd General Assembly PDFMa Luisa Oliva100% (1)
- Work From Home Accomplishment ReportDocument1 pageWork From Home Accomplishment ReportApril Dawn Daep100% (1)
- PRC Application for Crediting CPD ActivitiesDocument2 pagesPRC Application for Crediting CPD ActivitiesJerwin Cases Tiamson100% (3)
- DepEd Cotabato Oaths of OfficeDocument6 pagesDepEd Cotabato Oaths of OfficeNasra AbdulganiNo ratings yet
- Appendix 42 - Schedule of Unreleased ChecksDocument1 pageAppendix 42 - Schedule of Unreleased ChecksIvy Michelle HabagatNo ratings yet
- CS Form No. 4 Certification of Assumption To DutyDocument1 pageCS Form No. 4 Certification of Assumption To DutyludwigNo ratings yet
- CSC Appointment Processing ChecklistDocument1 pageCSC Appointment Processing ChecklistElmar Sillador50% (2)
- AAO Form 09142009-Revised IntongDocument1 pageAAO Form 09142009-Revised Intongmitch galax50% (2)
- School Records RequestDocument16 pagesSchool Records RequestAnge Line100% (1)
- Gender Sensitivity Training Pre-TestDocument2 pagesGender Sensitivity Training Pre-TestL'Michelli Kilayko HorladorNo ratings yet
- Got Talent Mechanics and CriteriaDocument1 pageGot Talent Mechanics and CriteriaJoanna Marie MenorNo ratings yet
- DSWD Purchase BookletDocument28 pagesDSWD Purchase BookletFermo Jr. Asufra100% (3)
- Parol Making Contest Criteria For JudgingDocument5 pagesParol Making Contest Criteria For JudgingTitser JeffNo ratings yet
- RER FormDocument4 pagesRER FormPam ElaNo ratings yet
- DBM CSC FormDocument4 pagesDBM CSC FormJing Goal Merit0% (1)
- Ara Form DDocument1 pageAra Form DKarissa0% (2)
- Form 33Document2 pagesForm 33Eduardo Yabut100% (1)
- Service Record TeacherDocument1 pageService Record TeacherMARCIAL ASADANo ratings yet
- PER-QF-04 POSITION DESCRIPTION FORM - CSC Revised 2017 (Administrative Assistant II (Disbursing Officer II)Document2 pagesPER-QF-04 POSITION DESCRIPTION FORM - CSC Revised 2017 (Administrative Assistant II (Disbursing Officer II)Lordiel Faderagao100% (1)
- Employee's Leave CardDocument10 pagesEmployee's Leave CardMarkNo ratings yet
- Acoustic Band Competition CriteriaDocument1 pageAcoustic Band Competition CriteriaPercival GuevarraNo ratings yet
- NSBI Guidelines OrientationDocument66 pagesNSBI Guidelines OrientationYza DelimaNo ratings yet
- Form 201 FilesDocument6 pagesForm 201 FilesNnayram Savir OllidapNo ratings yet
- BADMINTON MatrixDocument2 pagesBADMINTON MatrixMaricel Ayco0% (1)
- Reimbursement Expense ReceiptDocument1 pageReimbursement Expense ReceiptRamonitoElumbaring33% (3)
- Matti National High School Pass SlipDocument2 pagesMatti National High School Pass SlipSheila Bliss J. Goc-ongNo ratings yet
- ARA Form C of GsisDocument1 pageARA Form C of Gsisglenn padernalNo ratings yet
- Personnel Inventory Form: Contract of Services, Job Order And/or MOA City Government of DavaoDocument1 pagePersonnel Inventory Form: Contract of Services, Job Order And/or MOA City Government of DavaoIlyka Fe Paña100% (4)
- Flag Ceremony ScriptDocument3 pagesFlag Ceremony ScriptFrey Geo0% (1)
- Omnibus Certification of Authenticity and Veracity of DocumentsDocument3 pagesOmnibus Certification of Authenticity and Veracity of DocumentsLyn OlitaNo ratings yet
- 2023 Municipal Meet MemoDocument9 pages2023 Municipal Meet MemoRubeneva NunezNo ratings yet
- Municipal Pass Slip FormDocument3 pagesMunicipal Pass Slip FormMondster BatzNo ratings yet
- CS Form No. 32 Oath of OfficeDocument1 pageCS Form No. 32 Oath of OfficeBenjamin Fallado100% (1)
- Service Record FormDocument3 pagesService Record Formhersal fae gerardoNo ratings yet
- Timber City Academy Parental Consent Form for Annual School PageantDocument2 pagesTimber City Academy Parental Consent Form for Annual School PageantDandelion Kim Tutor MatildoNo ratings yet
- Surigaonon Basketball Club Basic Rules and Guidelines PDFDocument2 pagesSurigaonon Basketball Club Basic Rules and Guidelines PDFJefferson Niog86% (7)
- PTA Year-End Financial ReportDocument2 pagesPTA Year-End Financial ReportDecember Cool100% (1)
- Certification On Performance RatingDocument1 pageCertification On Performance RatingMaureen Mae EstanolNo ratings yet
- Teacher documents 2019Document2 pagesTeacher documents 2019Gener ToledoNo ratings yet
- Criteria Parol ContestDocument6 pagesCriteria Parol ContestBobby Leyco0% (1)
- ABAYON D. CERTIFICATE OF GOOD MORAL CHARACTER Grade 10 ADVISERS 2Document2 pagesABAYON D. CERTIFICATE OF GOOD MORAL CHARACTER Grade 10 ADVISERS 2A SiblingsNo ratings yet
- Criteria For Judging 2017Document3 pagesCriteria For Judging 2017Sui Ge Neris100% (1)
- CHORAL COMPETITION Diocese of Ilagan Parish Saint Joseph Choral GuidelinesDocument1 pageCHORAL COMPETITION Diocese of Ilagan Parish Saint Joseph Choral GuidelinesHarris Acoba100% (1)
- OMB Form 1 - Application For Ombudsman ClearanceDocument1 pageOMB Form 1 - Application For Ombudsman ClearanceMarlon Quimno100% (2)
- JHS Scholastic RecordDocument3 pagesJHS Scholastic RecordMylene N. MacedaNo ratings yet
- HOA - Certificate of No ObjectionDocument1 pageHOA - Certificate of No ObjectionClark Guilas100% (1)
- Prelim Judging: Criteria For Judging (Ginoo at Binibining Caramoran 2018)Document1 pagePrelim Judging: Criteria For Judging (Ginoo at Binibining Caramoran 2018)Pinkz Trinidad Talion100% (3)
- For Regulated AgenciesDocument2 pagesFor Regulated AgenciesAlexander Ligawad100% (3)
- CS Form No. 4 Certification of Assumption To DutyDocument1 pageCS Form No. 4 Certification of Assumption To DutyRic Laurence Sayson67% (6)
- Inventory and Inspection Report of Unserviceable PropertyDocument6 pagesInventory and Inspection Report of Unserviceable PropertyNestorJepolanCapiñaNo ratings yet
- Annex B List of PPEs Found at Station Malubog ESDocument4 pagesAnnex B List of PPEs Found at Station Malubog ESTintin Cadorna FielNo ratings yet
- Annex F RR 11-2018 (Sample)Document2 pagesAnnex F RR 11-2018 (Sample)amara corp100% (1)
- Explanation LetterDocument1 pageExplanation LetterMdrrmo Nabas100% (2)
- Policies On Leave-1Document55 pagesPolicies On Leave-10506shelton100% (3)
- Request For Withdrawal of GSIS Retirement Benefit Application FormatDocument1 pageRequest For Withdrawal of GSIS Retirement Benefit Application FormatLina Rhea0% (1)
- Revised 2012 FORMS A To EDocument11 pagesRevised 2012 FORMS A To Erotsacreijav66666No ratings yet
- For Agency Remittance Advice: FORM A. List of Employees With Life and Retirement PremiumDocument5 pagesFor Agency Remittance Advice: FORM A. List of Employees With Life and Retirement PremiumRodnieGubatonNo ratings yet
- SSS Employer Data Change Request Form R-8Document2 pagesSSS Employer Data Change Request Form R-8Jolas E. Brutas50% (2)
- Pep NotificationDocument3 pagesPep Notificationmathew1965No ratings yet
- 14 Rules For Writing Multiple-Choice QuestionsDocument2 pages14 Rules For Writing Multiple-Choice QuestionsGreg Terrones MuecoNo ratings yet
- 14 Rules For Writing Multiple-Choice QuestionsDocument5 pages14 Rules For Writing Multiple-Choice Questionsapi-322360160No ratings yet
- Activity Proposal SampleDocument2 pagesActivity Proposal SampleGreg Terrones Mueco86% (22)
- Action Research Work PlanDocument2 pagesAction Research Work PlanGreg Terrones MuecoNo ratings yet
- Raising Organizational Values Among TeachersDocument2 pagesRaising Organizational Values Among TeachersGreg Terrones Mueco100% (1)
- National Festival of Talents ProposalDocument3 pagesNational Festival of Talents ProposalGreg Terrones Mueco100% (3)
- Basic Encoding PDFDocument2 pagesBasic Encoding PDFGreg Terrones Mueco0% (1)
- SBM 2016 ApatDocument69 pagesSBM 2016 ApatGreg Terrones MuecoNo ratings yet
- Balanced Scorecard BasicsDocument3 pagesBalanced Scorecard BasicsCharminda RodrigoNo ratings yet
- Individual Plan For Professional Development (PPD)Document23 pagesIndividual Plan For Professional Development (PPD)Daisy MendiolaNo ratings yet
- Opcr and Ipcr-FormDocument217 pagesOpcr and Ipcr-FormGreg Terrones MuecoNo ratings yet
- Greg 1Document9 pagesGreg 1Greg Terrones MuecoNo ratings yet
- DepEd Form 18-E-1Document7 pagesDepEd Form 18-E-1lucdahNo ratings yet
- 514 Advances in Core ImageDocument126 pages514 Advances in Core ImageDiamond LewisNo ratings yet
- Module-I: Office Management and Automation - B. Com, FCMS, Sri Sri UniversityDocument52 pagesModule-I: Office Management and Automation - B. Com, FCMS, Sri Sri UniversityRamani RanjanNo ratings yet
- Accounts Maintenance - Salary Upload.22.08.2004Document2 pagesAccounts Maintenance - Salary Upload.22.08.2004yayabar4uNo ratings yet
- 08 GENEX Probe Operation For LTEDocument116 pages08 GENEX Probe Operation For LTEPhan An100% (1)
- The Citizen's Portal - Seven Seas TechnologiesDocument11 pagesThe Citizen's Portal - Seven Seas TechnologiesICT AUTHORITYNo ratings yet
- CS 8491 Computer ArchitectureDocument103 pagesCS 8491 Computer ArchitectureMUKESH KUMAR P 2019-2023 CSENo ratings yet
- What Is The 5G Charging Function?Document6 pagesWhat Is The 5G Charging Function?aliNo ratings yet
- 2-Accessories 23 July 2020Document6 pages2-Accessories 23 July 2020MohamedMahmoudNo ratings yet
- HP 3PAR StoreServe ELearning 1 2Q15 Full DeckDocument323 pagesHP 3PAR StoreServe ELearning 1 2Q15 Full Deckmjsmith11100% (2)
- Mid ServerDocument2 pagesMid ServerranjithgottimukkalaNo ratings yet
- Um3103 Stm32wba Nucleo64 Board mb1863 StmicroelectronicsDocument40 pagesUm3103 Stm32wba Nucleo64 Board mb1863 StmicroelectronicsslimslimkhmissiNo ratings yet
- TreeSize Professional - Folder Contents of - CDocument1 pageTreeSize Professional - Folder Contents of - CHenrique GilNo ratings yet
- Andrew Pakpahan - Installing and Configuring Freeradius + MySQL and Daloradius + MySQL On Ubuntu Server 12 PDFDocument7 pagesAndrew Pakpahan - Installing and Configuring Freeradius + MySQL and Daloradius + MySQL On Ubuntu Server 12 PDFZeref ANo ratings yet
- Unit 2 PythonDocument164 pagesUnit 2 Pythonviveksharma50011No ratings yet
- Menu - 634637063125928485 - CS6105 Compiler Design SyllabusDocument1 pageMenu - 634637063125928485 - CS6105 Compiler Design SyllabusArchit100% (1)
- Application Notes For Verbio TTS 9.10Document12 pagesApplication Notes For Verbio TTS 9.10supergauchoNo ratings yet
- Drawing ASCII ArtDocument3 pagesDrawing ASCII Artzeeshan0% (1)
- r19 C SyllabusDocument2 pagesr19 C SyllabusShaik ParveenNo ratings yet
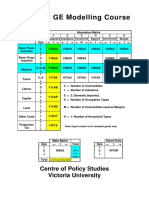
- Orani-G CourseDocument440 pagesOrani-G CourseVinícius Amaral100% (1)
- Oracle Cash ManagementDocument14 pagesOracle Cash ManagementCA Vara Reddy100% (2)
- 11-HTML-Iframes BSDKDocument3 pages11-HTML-Iframes BSDKBibek TripathyNo ratings yet
- Quarterly Report On The Physical Count of Property, Plant & Equipment (Rpcppe)Document2 pagesQuarterly Report On The Physical Count of Property, Plant & Equipment (Rpcppe)yelzyb100% (2)
- Ex 3 SRSDocument5 pagesEx 3 SRSVaibhav PuriNo ratings yet
- Learn To Hack WIFI Password With Ubuntu (WPA - WPA2)Document13 pagesLearn To Hack WIFI Password With Ubuntu (WPA - WPA2)Vigneshxbs50% (2)
- E.D.P.M Homework Sylvani CharlesDocument2 pagesE.D.P.M Homework Sylvani CharlesBlake KamminNo ratings yet
- Kaseya VSADocument12 pagesKaseya VSAVee SNo ratings yet
- SACS UtilitiesDocument45 pagesSACS UtilitiesUmar KidaNo ratings yet
- 2-32-1378907628-4. The Consumers .Full PDFDocument12 pages2-32-1378907628-4. The Consumers .Full PDFJaseem CTNo ratings yet
- Stranchat: Department of Computer Science, Christ UniversityDocument54 pagesStranchat: Department of Computer Science, Christ UniversityAryanKumarNo ratings yet
- Jupiter Installation Manual-ENG-v1 10-20170418Document21 pagesJupiter Installation Manual-ENG-v1 10-20170418David CazorlaNo ratings yet