You might also like
- RHYTHM CHEAT SHEET: A CONCISE GUIDEDocument1 pageRHYTHM CHEAT SHEET: A CONCISE GUIDEjb cookiesNo ratings yet
- EKG Quick and Dirty - GD v3.0Document2 pagesEKG Quick and Dirty - GD v3.0Sheema Sh100% (1)
- Spotlight On Cardiac DrugsDocument2 pagesSpotlight On Cardiac Drugspauerish100% (2)
- Nursing Diagnosis & Careplan SamplesDocument5 pagesNursing Diagnosis & Careplan SamplesE94% (18)
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesFrom EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesRating: 5 out of 5 stars5/5 (1)
- Digoxin: Andy Samelson's Drug Cards Andy Samelson's Drug CardsDocument57 pagesDigoxin: Andy Samelson's Drug Cards Andy Samelson's Drug Cardssplendidfender76% (17)
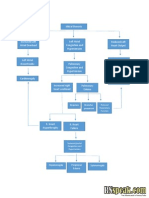
- Concept Map HypertensionDocument1 pageConcept Map Hypertensiongeorge pearson0% (1)
- FRACP Cardiology Study Notes Volume 1Document543 pagesFRACP Cardiology Study Notes Volume 1not here 2make friends sorryNo ratings yet
- Shock Comparison ChartDocument2 pagesShock Comparison Chartlinnaete88% (8)
- Drug CardsDocument10 pagesDrug CardsMaria Robustelli100% (3)
- Drug CardsDocument187 pagesDrug Cardsintaaf82% (33)
- Nursing Care Plan For Acute PainDocument5 pagesNursing Care Plan For Acute PainPhilippineNursingDirectory.com100% (9)
- Hypertension Concept MapDocument1 pageHypertension Concept Mapnursing concept maps100% (1)
- Concept Map COPDDocument2 pagesConcept Map COPDJilian McGugan88% (40)
- Dka Case Study Clinical ExampleDocument15 pagesDka Case Study Clinical ExampleVin Lorenzo Campbell100% (2)
- Drug Card LasixDocument2 pagesDrug Card LasixAdrianne Bazo100% (1)
- Nursing Head-to-Toe Assessment Cheat Sheet - Nurseslabs PDFDocument7 pagesNursing Head-to-Toe Assessment Cheat Sheet - Nurseslabs PDFNyeweh Sia Yomba67% (15)
- Nursing Care Plan Mobility SampleDocument6 pagesNursing Care Plan Mobility Samplen2biologyNo ratings yet
- Learning ECGDocument187 pagesLearning ECGPhysiology by Dr Raghuveer100% (2)
- Heart Failure COncept MapDocument2 pagesHeart Failure COncept MapJrBong SemaneroNo ratings yet
- Gerontological Nursing: Scope and Standards of Practice, 2nd EditionFrom EverandGerontological Nursing: Scope and Standards of Practice, 2nd EditionNo ratings yet
- IM SyllabusDocument7 pagesIM Syllabusepah1925100% (1)
- Chronic Kidney Disease: Bobby Laksana D Putri Priela Pembimbing: Dr. Nursamsu, SPPDDocument30 pagesChronic Kidney Disease: Bobby Laksana D Putri Priela Pembimbing: Dr. Nursamsu, SPPDfrostedsurgeonNo ratings yet
- ACS Nursing Care PlanDocument21 pagesACS Nursing Care Planchris_arc90100% (6)
- Ventricular ArrhythmiasDocument33 pagesVentricular ArrhythmiasSamantha DeshapriyaNo ratings yet
- Nursing DiagnosisDocument58 pagesNursing DiagnosisPrecious Santayana100% (3)
- Nursing Concept Map for Diabetes Patient ManagementDocument1 pageNursing Concept Map for Diabetes Patient ManagementSev Kuzmenko0% (1)
- Cirrohsis Case StudyDocument12 pagesCirrohsis Case Studykaitlynne lambertNo ratings yet
- Concept Map of DMDocument2 pagesConcept Map of DMLeslie Marie Rendon100% (9)
- Small Bowel Obstruction System - DisorderDocument1 pageSmall Bowel Obstruction System - DisorderMarina Wasem Netzlaff0% (1)
- Med Surge 2 - RESP SYSTEM NOTESDocument26 pagesMed Surge 2 - RESP SYSTEM NOTESlorrainenxumalo75% (4)
- COPD Care PLAN PDFDocument2 pagesCOPD Care PLAN PDFVanessaMUeller100% (1)
- Cardioversion & Defibrillation ExplainedDocument18 pagesCardioversion & Defibrillation ExplainedJannah Marie A. Dimaporo100% (4)
- Assessment and Management of Patients With Hearing and Balance Disorders WebDocument36 pagesAssessment and Management of Patients With Hearing and Balance Disorders WebStephKirstin Velasco Malapit100% (2)
- Small Bowel Obstruction Care PlanDocument11 pagesSmall Bowel Obstruction Care PlanKatie YarnellNo ratings yet
- PneumoniaDocument1 pagePneumonianursing concept mapsNo ratings yet
- COPD Risk Factors, Signs, Treatments & Nursing CareDocument2 pagesCOPD Risk Factors, Signs, Treatments & Nursing CareJilian McGugan100% (9)
- Lab Normal Value S&Sof S&Sof : Loma Linda University School of Nursing Accepted Lab Values Adapted From KaplanDocument3 pagesLab Normal Value S&Sof S&Sof : Loma Linda University School of Nursing Accepted Lab Values Adapted From KaplanGiacen100% (3)
- Bipolar Concept MapDocument3 pagesBipolar Concept Mapnursing concept maps100% (2)
- Concept Map StrokeDocument1 pageConcept Map StrokeMary GiuntiniNo ratings yet
- STUDENT-Eating - Disorder-F&E-UNFOLDING ReasoningDocument14 pagesSTUDENT-Eating - Disorder-F&E-UNFOLDING ReasoningPeggy100% (12)
- Congestive Heart Failure Schematic DiagramDocument1 pageCongestive Heart Failure Schematic DiagramCyrus De Asis100% (1)
- Hypertension Concept MapDocument1 pageHypertension Concept Mapgfhbgfhgf71% (7)
- Essential Stroke Nursing GuideDocument5 pagesEssential Stroke Nursing GuideAshleigh Johnstone100% (1)
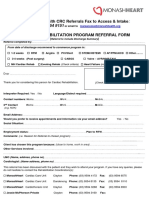
- CRP Referral Form 2016 Monash Heart V5Document1 pageCRP Referral Form 2016 Monash Heart V5Ansari JavedNo ratings yet
- Chronic Renal Failure: PathophysiologyDocument1 pageChronic Renal Failure: PathophysiologyCindy Mae Dela Torre100% (2)
- Concept MapDocument1 pageConcept MapChristine Marie Barce Martinez100% (2)
- Nursing Care Plan For "DYSRHYTHMIAS"Document12 pagesNursing Care Plan For "DYSRHYTHMIAS"jhonroks79% (14)
- ECG Library PDFDocument98 pagesECG Library PDFJayden WaveNo ratings yet
- Hemodialisis KdoqiDocument183 pagesHemodialisis KdoqiMaFer WueRa100% (2)
- Ventricular ArrhytmiaDocument30 pagesVentricular ArrhytmiaIkhsan AmadeaNo ratings yet
- Care Plan For Bowel ResectionDocument4 pagesCare Plan For Bowel Resectionviki840488% (8)
- Colon Cancer Case Study - 64yo Male Diagnosed After Rectal BleedingDocument2 pagesColon Cancer Case Study - 64yo Male Diagnosed After Rectal BleedingDragan Djordjevic100% (4)
- CHF Preparation QuestionsDocument6 pagesCHF Preparation Questionsgenium0689% (9)
- Cellulitis Care PlanDocument6 pagesCellulitis Care PlanNaya Kayala0% (1)
- Peripheral Vascular Disease NursingDocument13 pagesPeripheral Vascular Disease NursingCatlyn Chatpman100% (1)
- Careplan Concept MapDocument1 pageCareplan Concept MapAmanda Simpson100% (3)
- Managing Impaired Gas Exchange in an Elderly COPD PatientDocument23 pagesManaging Impaired Gas Exchange in an Elderly COPD PatientKaren Joyce Costales Magtanong100% (3)
- Concept Map Pleural EffusionDocument1 pageConcept Map Pleural Effusionapi-341263362No ratings yet
- Drugs WorksheetDocument16 pagesDrugs Worksheetninja-2001No ratings yet
- Cellulitis Concept MapDocument3 pagesCellulitis Concept MapBien EstrellaNo ratings yet
- Ricci KeithRN Eating DisorderDocument14 pagesRicci KeithRN Eating DisorderMichelle RicciNo ratings yet
- Intracranial HemorrhageDocument41 pagesIntracranial Hemorrhagedoctormussieaberra100% (1)
- CC-Concept Map 2Document5 pagesCC-Concept Map 2MDCITY50% (2)
- Congestive Heart Failure 1 Concept Map !Document1 pageCongestive Heart Failure 1 Concept Map !Franklin A. Salaum IIINo ratings yet
- TMendoza CriticalCareConceptMap2Document5 pagesTMendoza CriticalCareConceptMap2Theresa Fernandez Mendoza0% (1)
- Diuretic Drugs For Nursing PharmacologyDocument1 pageDiuretic Drugs For Nursing Pharmacologylhayes1234100% (7)
- Pacemakers & AICDs: What You Need to KnowDocument32 pagesPacemakers & AICDs: What You Need to KnowqmmmNo ratings yet
- Jihan Luqmannul Khakim, Dicky Aligheri Wartono, Bagus HerlambangDocument1 pageJihan Luqmannul Khakim, Dicky Aligheri Wartono, Bagus HerlambangazkacantikNo ratings yet
- Cardiac Arrhythmias in Africa: Epidemiology, Management Challenges, and PerspectivesDocument10 pagesCardiac Arrhythmias in Africa: Epidemiology, Management Challenges, and PerspectivesmahsusiyatiNo ratings yet
- Pilipinas: Miss Philippines of Michigan 2008 PageantDocument12 pagesPilipinas: Miss Philippines of Michigan 2008 Pageantstevec74100% (3)
- Acute Coronary Syndrome in Clinical Practice: Firman B. LeksmonoDocument48 pagesAcute Coronary Syndrome in Clinical Practice: Firman B. Leksmonojames klemens phieter phieNo ratings yet
- Etik Dwi Ningsih, Indah Mukarromah, Athi' L Inda YaniDocument9 pagesEtik Dwi Ningsih, Indah Mukarromah, Athi' L Inda YaniMuhamad fajarNo ratings yet
- Nama Nama Yang Tidak Mengumpulkan Soal Ujian Utb 4.1: Akademik Roften CardioDocument8 pagesNama Nama Yang Tidak Mengumpulkan Soal Ujian Utb 4.1: Akademik Roften CardioSyaffira SalsabilaNo ratings yet
- Lifepak CR Plus BrochureDocument20 pagesLifepak CR Plus BrochurenugiexNo ratings yet
- Inter-Rater Reliability of ST-Segment Measurement at A University Hospital in ArgentinaDocument4 pagesInter-Rater Reliability of ST-Segment Measurement at A University Hospital in ArgentinaSholehuddin MunajjidNo ratings yet
- CVS - Charts & DiagramsDocument20 pagesCVS - Charts & DiagramsMamathaNo ratings yet
- 2020 Eagle Practical CardiologyDocument24 pages2020 Eagle Practical CardiologyaeliasgvNo ratings yet
- GlomerulonephritisDocument1 pageGlomerulonephritismaleskunNo ratings yet
- Program SPCCTV 2019 CardiacSurgeryDocument8 pagesProgram SPCCTV 2019 CardiacSurgeryDu SantosNo ratings yet
- Non St-Segment Elevation Acute Coronary Syndrome (Nste-Acs) : EtiologyDocument4 pagesNon St-Segment Elevation Acute Coronary Syndrome (Nste-Acs) : EtiologyKEn PilapilNo ratings yet
- Daftar PustakaDocument9 pagesDaftar PustakaEvan DionesiaNo ratings yet
- Ecg TeachingDocument44 pagesEcg TeachingarvindkanagaratnamNo ratings yet
- Adams-Stokes 1º Sintoma Febre ReumáticaDocument5 pagesAdams-Stokes 1º Sintoma Febre Reumáticacarvalho.tr4270No ratings yet
- Acute Kidney Injury - Mini Lecture: Updated 02/2013Document11 pagesAcute Kidney Injury - Mini Lecture: Updated 02/2013Asmalina AzizanNo ratings yet