You might also like
- E M HW4v3 A2 001 - 10Document25 pagesE M HW4v3 A2 001 - 10hsingnan.instrumentNo ratings yet
- 17 Procedure Equipment Maintenance Measuring Equipment Integrated Preview ENDocument3 pages17 Procedure Equipment Maintenance Measuring Equipment Integrated Preview ENMohamed RafeeNo ratings yet
- ECA Virtual IT Systems in A GXP EnvironmentDocument4 pagesECA Virtual IT Systems in A GXP EnvironmentHemant GoswamiNo ratings yet
- GMP Module - Data IntegrityDocument46 pagesGMP Module - Data Integritydeepa_ragu5695No ratings yet
- Cardinal Health Gs1 Implementation Guide 1 2Document126 pagesCardinal Health Gs1 Implementation Guide 1 2Hazem FaroukNo ratings yet
- Cleaning ValidationDocument9 pagesCleaning ValidationChirag PatelNo ratings yet
- SIP Project of VSMDocument77 pagesSIP Project of VSMPrasad BachhavNo ratings yet
- Ilovepdf Merged PDFDocument25 pagesIlovepdf Merged PDFSf BztprkNo ratings yet
- Data IntegrityDocument14 pagesData IntegritysanjitlNo ratings yet
- Life Sciences Building Management Solutions BrochureDocument16 pagesLife Sciences Building Management Solutions BrochureSimon MadreadoNo ratings yet
- FDA CFR 806 Format PDFDocument2 pagesFDA CFR 806 Format PDFSriNo ratings yet
- WWW - Unlock PDF - Com JAKAR SOP 000216Document25 pagesWWW - Unlock PDF - Com JAKAR SOP 000216kenangNo ratings yet
- ISBT Guidelines For Validation of Automated Systems in Blood Establishments PDFDocument25 pagesISBT Guidelines For Validation of Automated Systems in Blood Establishments PDFGloryNo ratings yet
- Oman Labour LawDocument35 pagesOman Labour Lawraghu.cecri8058100% (1)
- Tools & Techniques in Quality Dept 2004 09 23Document4 pagesTools & Techniques in Quality Dept 2004 09 23BaljeetNo ratings yet
- Mostafa Mahmoud Soliman CV - March 2023Document5 pagesMostafa Mahmoud Soliman CV - March 2023Mustafa Mahmoud MatarNo ratings yet
- Project Charter TemplateDocument3 pagesProject Charter TemplateSarvesh DaradeNo ratings yet
- Mandatory Problem ReportingDocument24 pagesMandatory Problem ReportingTZ LABNo ratings yet
- CompleteDRGD With Appendices Update July15 PDFDocument662 pagesCompleteDRGD With Appendices Update July15 PDFcatherinegohNo ratings yet
- QM0492 Quality Manual-BEDocument55 pagesQM0492 Quality Manual-BEBC EimorNo ratings yet
- Getinge Hs5510-Single-Door-SterilizerDocument8 pagesGetinge Hs5510-Single-Door-Sterilizermohd shuib abd rahmanNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument12 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNAL100% (1)
- Sample 02 - Strategic Change Management - CompressedDocument17 pagesSample 02 - Strategic Change Management - CompressedSadaf YousafNo ratings yet
- VHP DCA Technical Data Sheet PDFDocument8 pagesVHP DCA Technical Data Sheet PDFMohammed AltafNo ratings yet
- Iata Ceiv-Pharma How20to20become20ceiv20pharma20certifiedDocument132 pagesIata Ceiv-Pharma How20to20become20ceiv20pharma20certifiedAdmin OPS APLOG KPNo ratings yet
- EU Directory of Regulations and Standards PDFDocument16 pagesEU Directory of Regulations and Standards PDFanon_684099349No ratings yet
- Issuance of DocumentsDocument2 pagesIssuance of DocumentsAshok KumarNo ratings yet
- FeasibilityDocument8 pagesFeasibilityOTNo ratings yet
- ISO 22000 - 2018 A Brief OverviewDocument28 pagesISO 22000 - 2018 A Brief OverviewGenNo ratings yet
- FDA-ISO QMS Audit Checklist GreenlightDocument3 pagesFDA-ISO QMS Audit Checklist Greenlightada wangNo ratings yet
- AeroTrak - Plus - A100 31 35 50 51 55 - APC - User Manual 6016408 - USDocument74 pagesAeroTrak - Plus - A100 31 35 50 51 55 - APC - User Manual 6016408 - USRezaul KarimNo ratings yet
- Session 14 Train Personnel On CSV and Data Integrity ComplianceDocument36 pagesSession 14 Train Personnel On CSV and Data Integrity ComplianceAl RammohanNo ratings yet
- Job Description For KPMGDocument1 pageJob Description For KPMGDulcet LyricsNo ratings yet
- PDF Test Medical Nitrile Exam GloveDocument13 pagesPDF Test Medical Nitrile Exam GloveRicha RohillaNo ratings yet
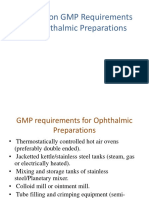
- Seminar On GMP Requirements For Ophthalmic PreparationsDocument57 pagesSeminar On GMP Requirements For Ophthalmic Preparationsvkguptajss100% (1)
- VK 7000-7010-750D Dissolution Tester Qualification GuideDocument175 pagesVK 7000-7010-750D Dissolution Tester Qualification GuideJhon Edison Briceño PeñuelaNo ratings yet
- GD Gdpmds Draft1Document24 pagesGD Gdpmds Draft1Syaiful NazwanNo ratings yet
- ISO 14001 Administrative Flowchart ExamplesDocument17 pagesISO 14001 Administrative Flowchart ExamplesPercy MphulanyaneNo ratings yet
- Guidelines On Validation - Appendix 5 2Document1 pageGuidelines On Validation - Appendix 5 2nagarajs50No ratings yet
- Japan QMS Whitepaper EmergoDocument9 pagesJapan QMS Whitepaper EmergoGuillaumeNo ratings yet
- 49-2019 Annex1Document45 pages49-2019 Annex1CataNo ratings yet
- Session1 Gunning Vidya PresDocument21 pagesSession1 Gunning Vidya PresRama ReddyNo ratings yet
- Airlines Reservation System: ISBM University, Nawapara (Kosmi), Block & Tehsil - Chhura, District - Gariyaband (C.G.)Document5 pagesAirlines Reservation System: ISBM University, Nawapara (Kosmi), Block & Tehsil - Chhura, District - Gariyaband (C.G.)Aashish JoshiNo ratings yet
- India Glycols Limited: An Industrial Training Report ofDocument48 pagesIndia Glycols Limited: An Industrial Training Report ofVishwaraj0% (1)
- Gen Audit Check InterimguidanceDocument38 pagesGen Audit Check InterimguidanceKristabel Wenardi100% (1)
- Lab-Systems Application Server Details-2.0Document37 pagesLab-Systems Application Server Details-2.0Billa SathishNo ratings yet
- Annex IV Part IV Audit Report Template v4.1 PDFDocument6 pagesAnnex IV Part IV Audit Report Template v4.1 PDFMichael FadjarNo ratings yet
- Technical Requirements in Vitro Diagnostics (IVD)Document4 pagesTechnical Requirements in Vitro Diagnostics (IVD)Raydoon Sadeq100% (1)
- Delivery Report: Delivering DealerDocument2 pagesDelivery Report: Delivering DealerBrayan Calcina BellotNo ratings yet
- SCADA Operator InterfaceDocument148 pagesSCADA Operator Interfacejatupon prasuradNo ratings yet
- HARPS Example Glass and Hard Plastic RegisterDocument1 pageHARPS Example Glass and Hard Plastic RegisterDaniel ModicaNo ratings yet
- Corporate, IQA Observation SheetDocument2 pagesCorporate, IQA Observation SheetSachin RamdurgNo ratings yet
- Example ASTM 6319 Test ReportDocument7 pagesExample ASTM 6319 Test ReportNathan NadavNo ratings yet
- Autoclave CycleDocument7 pagesAutoclave CycleHaroon RasheedNo ratings yet
- Hid Support HandbookDocument46 pagesHid Support HandbookChance Christian100% (1)
- E2open 2021 Forecasting and Inventory Benchmark Study Full ReportDocument48 pagesE2open 2021 Forecasting and Inventory Benchmark Study Full ReportdbrenesvNo ratings yet
- Mean Kinetic Temperature (MKT) in Stability Studies - Pharmaceutical GuidelinesDocument1 pageMean Kinetic Temperature (MKT) in Stability Studies - Pharmaceutical Guidelinesitung23No ratings yet
- Iso 9187 1 1991Document9 pagesIso 9187 1 1991Muhammad ImranNo ratings yet
- FAT-Compounding Isolator 100 L Compounding VesselDocument33 pagesFAT-Compounding Isolator 100 L Compounding Vesseldhanu_lagwankarNo ratings yet
- MasterCard Muslim IndexDocument38 pagesMasterCard Muslim IndexshinkoicagmailcomNo ratings yet
- Eid Celebrations in Qatar 2016 - Schedule & MapDocument2 pagesEid Celebrations in Qatar 2016 - Schedule & Mapshabina921No ratings yet
- WEF Human Capital Report 2015 - QatarDocument2 pagesWEF Human Capital Report 2015 - Qatarshabina921No ratings yet
- The U.S. State Department Removed Cuba and Malaysia From Its Human Trafficking BlacklistDocument384 pagesThe U.S. State Department Removed Cuba and Malaysia From Its Human Trafficking BlacklistBarbara EspinosaNo ratings yet
- Bayt Job Satisfaction Report 04 2015Document62 pagesBayt Job Satisfaction Report 04 2015shabina921No ratings yet
- Mowasalat Bus RouteDocument1 pageMowasalat Bus Routeshabina92129% (7)
- KamranDocument1 pageKamranshabina921No ratings yet
- Katara National Day Activities 2014Document3 pagesKatara National Day Activities 2014shabina921No ratings yet
- Sports Village ScheduleDocument5 pagesSports Village Scheduleshabina921No ratings yet
- October Statistics - Ministry of Development, Planning and StatisticsDocument24 pagesOctober Statistics - Ministry of Development, Planning and Statisticsshabina921No ratings yet
- CPI BrochureDocument12 pagesCPI BrochureRashi MathurNo ratings yet
- CITES Cheetah ReportDocument54 pagesCITES Cheetah Reportshabina921No ratings yet
- Home Rental Rates and Affordability in QatarDocument12 pagesHome Rental Rates and Affordability in Qatarshabina921No ratings yet
- Qatar Monthly Statistics July 2014 Edition 6Document22 pagesQatar Monthly Statistics July 2014 Edition 6shabina921No ratings yet
- FIFA Ethics StatementDocument42 pagesFIFA Ethics Statementshabina921No ratings yet
- Children and Women ReportDocument236 pagesChildren and Women Reportshabina921No ratings yet
- Qatar Monthly Statistics Edition 8 For Web 2Document21 pagesQatar Monthly Statistics Edition 8 For Web 2shabina921No ratings yet
- WWF Living Planet Report 2014Document180 pagesWWF Living Planet Report 2014ishmael daroNo ratings yet
- Qatar Tourism Authority Mall Entertainment ScheduleDocument1 pageQatar Tourism Authority Mall Entertainment Scheduleshabina921No ratings yet
- Qatar Monthly Statistics July 2014 Edition 6Document22 pagesQatar Monthly Statistics July 2014 Edition 6shabina921No ratings yet
- EN Draft E-Participation PolicyDocument59 pagesEN Draft E-Participation Policyshabina921No ratings yet
- 2014 Human Development Report English PDFDocument239 pages2014 Human Development Report English PDFMiguel BenedettiNo ratings yet
- InterNations Survey Report Top Expat Destinations 2014 PDFDocument197 pagesInterNations Survey Report Top Expat Destinations 2014 PDFcaidas_libresNo ratings yet
- Qatar Monthly Statistics August 2014 Edition 7Document22 pagesQatar Monthly Statistics August 2014 Edition 7shabina921No ratings yet
- Household Expenditure EngDocument206 pagesHousehold Expenditure Engshabina921No ratings yet
- Migrant Labour Recruitment To QatarDocument162 pagesMigrant Labour Recruitment To Qatarshabina921100% (1)
- Qatar Monthly Statistics Edition 5 For PrintDocument24 pagesQatar Monthly Statistics Edition 5 For Printshabina921No ratings yet
- GCC Education Industry Report July 2014Document97 pagesGCC Education Industry Report July 2014shabina921No ratings yet
- Capital Projects Survey 2014Document28 pagesCapital Projects Survey 2014shabina921No ratings yet
- Global Islamic Economy ReportDocument220 pagesGlobal Islamic Economy ReportYusufArieNo ratings yet
- David F. DeRosa - Central Banking and Monetary Policy in Emerging-Markets Nations (2009)Document176 pagesDavid F. DeRosa - Central Banking and Monetary Policy in Emerging-Markets Nations (2009)Deanne GuintoNo ratings yet
- A98 - Case-Edita-Foods PDFDocument17 pagesA98 - Case-Edita-Foods PDFMD Saiful IslamNo ratings yet
- Currencies A PrimerDocument15 pagesCurrencies A PrimerNicolae VutcariovNo ratings yet
- Global People Paradigm - Shifting The Frontier of People ManagementDocument48 pagesGlobal People Paradigm - Shifting The Frontier of People ManagementFarukHosenRajNo ratings yet
- Mishkin Econ13e PPT 17Document25 pagesMishkin Econ13e PPT 17Huyền Nhi QuảnNo ratings yet
- A Test of The International Fisher Effect in Selected Asian CountriesDocument7 pagesA Test of The International Fisher Effect in Selected Asian CountriesCARLOS RODRIGUEZNo ratings yet
- CFP Introduction To Financial Planning Study Notes SampleDocument42 pagesCFP Introduction To Financial Planning Study Notes SampleMeenakshi67% (3)
- Chapter 10Document14 pagesChapter 10Zhang XuantaoNo ratings yet
- MacDonald &dias - Behavioural Equilibrium Exchange Rate Estimates and Implied Exchange Rate Adjustments For Ten CountriesDocument33 pagesMacDonald &dias - Behavioural Equilibrium Exchange Rate Estimates and Implied Exchange Rate Adjustments For Ten Countrieskhrysttalexa3146No ratings yet
- International Parity Relationships & Forecasting Exchange RatesDocument33 pagesInternational Parity Relationships & Forecasting Exchange RatesKARISHMAATA2No ratings yet
- Quiz 2 ECODocument2 pagesQuiz 2 ECOEugene AlipioNo ratings yet
- Dissertation, Gaurav Goyal, A1210208A17, A 1210204020Document119 pagesDissertation, Gaurav Goyal, A1210208A17, A 1210204020mundawala_sgnrNo ratings yet
- Blade Inc CaseDocument11 pagesBlade Inc Caserasha_fayez60% (5)
- (K55CLC1 - GROUP 7) How Could Market Imperfection Affect Interest Rate ParityDocument29 pages(K55CLC1 - GROUP 7) How Could Market Imperfection Affect Interest Rate ParityTrần TuyềnNo ratings yet
- The Rise and Fall of American Hegemony From Wilson To TrumpDocument18 pagesThe Rise and Fall of American Hegemony From Wilson To TrumpNicolás TerradasNo ratings yet
- Macroeconomics 12th Edition Michael Parkin Solutions Manual 1Document14 pagesMacroeconomics 12th Edition Michael Parkin Solutions Manual 1ka100% (43)
- API NY - GDP.PCAP - PP.CD DS2 en Excel v2 167Document56 pagesAPI NY - GDP.PCAP - PP.CD DS2 en Excel v2 167syasya tanNo ratings yet
- Module MAF Int Finance 2020Document40 pagesModule MAF Int Finance 2020simoneNo ratings yet
- Tutorial 4 Exercises IFMDocument5 pagesTutorial 4 Exercises IFMNguyễn Gia Phương Anh100% (1)
- Irpt & PPPTDocument3 pagesIrpt & PPPTKhabele LenkoeNo ratings yet
- FOREX MARKETS Part 3Document31 pagesFOREX MARKETS Part 3Parvesh AghiNo ratings yet
- Dissertation On Foreign Exchange RateDocument6 pagesDissertation On Foreign Exchange RatePaySomeoneToWriteYourPaperHighPoint100% (1)
- Ch10 Thomson Answers To QuestionsDocument6 pagesCh10 Thomson Answers To Questionsgeorgeterekhov100% (1)
- Madura14e Ch08 FinalDocument38 pagesMadura14e Ch08 FinalfabianngxinlongNo ratings yet
- Headey e Ecker 2013Document17 pagesHeadey e Ecker 2013grazielaNo ratings yet
- The Transition From Barter Trade To Impediments of The Dollar System: One Nation, One Currency, One MonopolyDocument34 pagesThe Transition From Barter Trade To Impediments of The Dollar System: One Nation, One Currency, One MonopolyJohn TaskinsoyNo ratings yet
- Purchasing Power Parity TheoryDocument10 pagesPurchasing Power Parity TheoryPrakash RaiNo ratings yet
- Gross Domestic ProductDocument8 pagesGross Domestic ProductNiño Rey LopezNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- EMT (Emergency Medical Technician) Crash Course with Online Practice Test, 2nd Edition: Get a Passing Score in Less TimeFrom EverandEMT (Emergency Medical Technician) Crash Course with Online Practice Test, 2nd Edition: Get a Passing Score in Less TimeRating: 3.5 out of 5 stars3.5/5 (3)
- Preclinical Pathology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Pathology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Rating: 5 out of 5 stars5/5 (1)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- The NCLEX-RN Exam Study Guide: Premium Edition: Proven Methods to Pass the NCLEX-RN Examination with Confidence – Extensive Next Generation NCLEX (NGN) Practice Test Questions with AnswersFrom EverandThe NCLEX-RN Exam Study Guide: Premium Edition: Proven Methods to Pass the NCLEX-RN Examination with Confidence – Extensive Next Generation NCLEX (NGN) Practice Test Questions with AnswersNo ratings yet
- Improve Your Global Business English: The Essential Toolkit for Writing and Communicating Across BordersFrom EverandImprove Your Global Business English: The Essential Toolkit for Writing and Communicating Across BordersRating: 4 out of 5 stars4/5 (14)
- The Official U.S. Army Survival Guide: Updated Edition: FM 30-05.70 (FM 21-76)From EverandThe Official U.S. Army Survival Guide: Updated Edition: FM 30-05.70 (FM 21-76)Rating: 4 out of 5 stars4/5 (1)
- USMLE Step 1: Integrated Vignettes: Must-know, high-yield reviewFrom EverandUSMLE Step 1: Integrated Vignettes: Must-know, high-yield reviewRating: 4.5 out of 5 stars4.5/5 (7)
- Outliers by Malcolm Gladwell - Book Summary: The Story of SuccessFrom EverandOutliers by Malcolm Gladwell - Book Summary: The Story of SuccessRating: 4.5 out of 5 stars4.5/5 (17)
- Nursing School Entrance Exams: HESI A2 / NLN PAX-RN / PSB-RN / RNEE / TEASFrom EverandNursing School Entrance Exams: HESI A2 / NLN PAX-RN / PSB-RN / RNEE / TEASNo ratings yet
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyRating: 4 out of 5 stars4/5 (18)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (6)
- Note Taking Mastery: How to Supercharge Your Note Taking Skills & Study Like a GeniusFrom EverandNote Taking Mastery: How to Supercharge Your Note Taking Skills & Study Like a GeniusRating: 3.5 out of 5 stars3.5/5 (10)
- NASM CPT Study Guide 2024-2025: Review Book with 360 Practice Questions and Answer Explanations for the Certified Personal Trainer ExamFrom EverandNASM CPT Study Guide 2024-2025: Review Book with 360 Practice Questions and Answer Explanations for the Certified Personal Trainer ExamNo ratings yet
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- Pilot's Handbook of Aeronautical Knowledge (2024): FAA-H-8083-25CFrom EverandPilot's Handbook of Aeronautical Knowledge (2024): FAA-H-8083-25CNo ratings yet
- 1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideFrom Everand1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideRating: 3.5 out of 5 stars3.5/5 (7)
- Norman Hall's Firefighter Exam Preparation BookFrom EverandNorman Hall's Firefighter Exam Preparation BookRating: 5 out of 5 stars5/5 (3)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- The CompTIA Network+ & Security+ Certification: 2 in 1 Book- Simplified Study Guide Eighth Edition (Exam N10-008) | The Complete Exam Prep with Practice Tests and Insider Tips & Tricks | Achieve a 98% Pass Rate on Your First Attempt!From EverandThe CompTIA Network+ & Security+ Certification: 2 in 1 Book- Simplified Study Guide Eighth Edition (Exam N10-008) | The Complete Exam Prep with Practice Tests and Insider Tips & Tricks | Achieve a 98% Pass Rate on Your First Attempt!No ratings yet