You might also like
- ISS Packet Operation On 70cm-20161113Document1 pageISS Packet Operation On 70cm-20161113tom2susanNo ratings yet
- The Kit Carson TrailDocument4 pagesThe Kit Carson Trailtom2susanNo ratings yet
- Chokes and Shot PatternDocument5 pagesChokes and Shot Patterntom2susanNo ratings yet
- Enron: The Good, The Bad, The LessonsDocument20 pagesEnron: The Good, The Bad, The Lessonstom2susanNo ratings yet
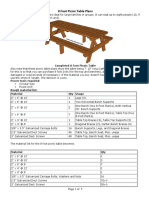
- 8 Foot Picnic Table PlansDocument5 pages8 Foot Picnic Table Planstom2susanNo ratings yet
- Bandanas Carryout MenuDocument3 pagesBandanas Carryout Menutom2susanNo ratings yet
- BabbosDocument2 pagesBabbostom2susanNo ratings yet
- Cloud ChartDocument2 pagesCloud Charttom2susanNo ratings yet
- Panera 2018Document4 pagesPanera 2018tom2susanNo ratings yet
- Thyroid Nodules TI-RADSDocument1 pageThyroid Nodules TI-RADStom2susanNo ratings yet
- Federal Explosives Law and Regulations 2012 Atf-P-5400-7 PDFDocument112 pagesFederal Explosives Law and Regulations 2012 Atf-P-5400-7 PDFtom2susanNo ratings yet
- Cansat2017 5235 CDR v02Document185 pagesCansat2017 5235 CDR v02tom2susanNo ratings yet
- Bennett Spring Hatch ChartDocument1 pageBennett Spring Hatch Charttom2susanNo ratings yet
- ABI CodingDocument2 pagesABI Codingtom2susanNo ratings yet
- Arduino For Ham Radio PresentationDocument50 pagesArduino For Ham Radio Presentationtom2susan100% (2)
- VA Housebound Form VBA-21-2680Document2 pagesVA Housebound Form VBA-21-2680tom2susanNo ratings yet
- Blue CardDocument1 pageBlue Cardtom2susanNo ratings yet
- Va Home Health Care InformationDocument2 pagesVa Home Health Care Informationtom2susanNo ratings yet
- Therapeutic Shoes For Persons With Diabetes PresentationDocument67 pagesTherapeutic Shoes For Persons With Diabetes Presentationtom2susanNo ratings yet
- 2015 AMMC (SUMMER) Student HandoutDocument84 pages2015 AMMC (SUMMER) Student Handouttom2susanNo ratings yet
- Animal Science PowerpointDocument104 pagesAnimal Science Powerpointtom2susanNo ratings yet
- Pyrotechnics - Weingart 1947 PDFDocument247 pagesPyrotechnics - Weingart 1947 PDFtom2susanNo ratings yet
- SB 656 PassedDocument49 pagesSB 656 Passedtom2susanNo ratings yet
- Personal Fitness MBDocument14 pagesPersonal Fitness MBtom2susanNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Soil Contamination With Cadmium, Consequences and Remediation UsingDocument15 pagesSoil Contamination With Cadmium, Consequences and Remediation UsingsalmanNo ratings yet
- Radiologi Intervensi Di IndiaDocument3 pagesRadiologi Intervensi Di IndiaPutu Adi SusantaNo ratings yet
- Atlas de AcupunturaDocument258 pagesAtlas de AcupunturaPatricia Barrera100% (2)
- Mental Health DirectoryDocument88 pagesMental Health DirectoryAbhijit DasNo ratings yet
- USHK - A - Clean - Environment - Healthy - Me - EngDocument24 pagesUSHK - A - Clean - Environment - Healthy - Me - EngBeaa BeaaNo ratings yet
- Food Safety Officer and Technical Officer FSSAI Guide 2019 PDFDocument15 pagesFood Safety Officer and Technical Officer FSSAI Guide 2019 PDFChinmoy Das0% (5)
- BCAAs and Body Composition - Art de Vany On LineDocument2 pagesBCAAs and Body Composition - Art de Vany On LineDellNo ratings yet
- Cl2 Material Safety Data SheetDocument11 pagesCl2 Material Safety Data SheetChristian CoboNo ratings yet
- Shafers Textbook of Oral Pathology 9Th Edition William G Shafer All ChapterDocument67 pagesShafers Textbook of Oral Pathology 9Th Edition William G Shafer All Chaptermary.graham20483% (6)
- Prof Rika - Konsep Dasar Biologi Sel Dan MolekularDocument33 pagesProf Rika - Konsep Dasar Biologi Sel Dan MolekularTiaradestiana AbeeNo ratings yet
- Bonus BooksDocument540 pagesBonus BooksDanielle Moore100% (2)
- Saudi License Exam (SLE) For General Dentistry - Sep 6, 2011Document10 pagesSaudi License Exam (SLE) For General Dentistry - Sep 6, 2011asifhameed90% (10)
- Barneys Farm SeedsDocument46 pagesBarneys Farm SeedsPedro MarquesNo ratings yet
- Street Corner Secrets by Svati ShahDocument71 pagesStreet Corner Secrets by Svati ShahDuke University Press100% (2)
- Natrum Muriaticum - Materia Medica by James Tyler Kent, A.m., M.DDocument1 pageNatrum Muriaticum - Materia Medica by James Tyler Kent, A.m., M.DJayNo ratings yet
- The Effect of Physiotherapy Intervention by Using Ultrasound and Piriformis Stretching in Management To Reduce Pain in Piriformis SyndromeDocument3 pagesThe Effect of Physiotherapy Intervention by Using Ultrasound and Piriformis Stretching in Management To Reduce Pain in Piriformis SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- OB TriageDocument36 pagesOB TriagerelinNo ratings yet
- American Family PhysicianDocument4 pagesAmerican Family PhysicianGoddess Nth The Artemis EffectNo ratings yet
- Toshiba Xario XG User ManualDocument25 pagesToshiba Xario XG User ManualSalah AnamNo ratings yet
- TURP SyndromeDocument13 pagesTURP SyndromeWindy Ari WijayaNo ratings yet
- 4biomechanics of Removable Partial DenturesDocument15 pages4biomechanics of Removable Partial DenturesDemilyadioppy AbevitNo ratings yet
- Mechanisms of Ageing and Development: SciencedirectDocument8 pagesMechanisms of Ageing and Development: SciencedirectAgustin LopezNo ratings yet
- Traditional Healers in South AfricaDocument8 pagesTraditional Healers in South AfricaTraditional Healer100% (1)
- Digestive System Charts 1Document14 pagesDigestive System Charts 1api-306762527No ratings yet
- Accreditation and Certification 10 09Document2 pagesAccreditation and Certification 10 09Snegha RajaNo ratings yet
- Reactive ArthritisDocument8 pagesReactive ArthritisamereNo ratings yet
- Cellular Detox Smoothies PDFDocument20 pagesCellular Detox Smoothies PDFRuth Engelthaler100% (3)
- MCN ReviewerDocument5 pagesMCN ReviewerJunghoon YangParkNo ratings yet
- One Health ConceptDocument2 pagesOne Health ConceptYume AkamaiNo ratings yet
- Lecture 5 - Facial Pain and TMJ DiseaseDocument6 pagesLecture 5 - Facial Pain and TMJ DiseaseJeff ChadwickNo ratings yet