You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Artist Management Contract - Doc1Document5 pagesArtist Management Contract - Doc1Angela PaduaNo ratings yet
- Evoe Spring Spa: A Positioning Dilemma: Presented byDocument7 pagesEvoe Spring Spa: A Positioning Dilemma: Presented byHimanish BhandariNo ratings yet
- Consumer Buying Behavior of Consumers Towards NestleDocument4 pagesConsumer Buying Behavior of Consumers Towards NestleAli Akram100% (3)
- Janki Main Project (Skoda)Document88 pagesJanki Main Project (Skoda)trushna190% (4)
- Define NeedsDocument2 pagesDefine NeedsSabikosyaNo ratings yet
- Sugar Free CaseDocument14 pagesSugar Free CaseVimal Singh ChauhanNo ratings yet
- Online Advertising BLUE BOOK: The Guide To Ad Networks & ExchangesDocument28 pagesOnline Advertising BLUE BOOK: The Guide To Ad Networks & ExchangesmThink100% (1)
- Monocle: Throwing A Lifeline To A Struggling Manufacturing SectorDocument6 pagesMonocle: Throwing A Lifeline To A Struggling Manufacturing SectorReal Fabrica Española100% (1)
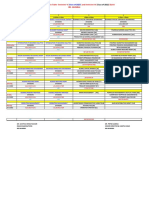
- End-Term Exam Time Table - Feb 2022Document2 pagesEnd-Term Exam Time Table - Feb 2022Avinaba GuhaNo ratings yet
- Xiomi File 3Document50 pagesXiomi File 3nirali100% (1)
- Training Program PlanDocument16 pagesTraining Program Planapi-277710124No ratings yet
- Chapter - 1Document93 pagesChapter - 1sheleftmeNo ratings yet
- HR Competency Models Through the YearsDocument17 pagesHR Competency Models Through the YearsSoumyajit PradhanNo ratings yet
- QMR Assignment Single and Ambitious: Tushar GuptaDocument5 pagesQMR Assignment Single and Ambitious: Tushar Guptabinzidd007No ratings yet
- Brandon ClayshootDocument1 pageBrandon ClayshootbgctampaNo ratings yet
- Value Networks & Marketing Channels ExplainedDocument8 pagesValue Networks & Marketing Channels ExplainedSønder SøulNo ratings yet
- Marketing Unit 1Document38 pagesMarketing Unit 1Ritika AroraNo ratings yet
- 2nd Quarter Exam EntrepreneurshipDocument5 pages2nd Quarter Exam Entrepreneurshipjeo nalugon100% (1)
- Export DocumentationDocument36 pagesExport Documentationpura_malliNo ratings yet
- Grade 6-Pretest On ComsumerDocument17 pagesGrade 6-Pretest On ComsumerAndrea Jarani LinezoNo ratings yet
- MBA Ethics Exam Questions on Business FraudDocument9 pagesMBA Ethics Exam Questions on Business FraudVrinda GopinathNo ratings yet
- Optimal Control and Dynamic Games PDFDocument351 pagesOptimal Control and Dynamic Games PDFNailulNellyIzzatiNo ratings yet
- Term Report Surf ExcelDocument27 pagesTerm Report Surf Excelbaigfaheem100% (3)
- 4ueo 637921 654246Document21 pages4ueo 637921 654246wendy panNo ratings yet
- Professional Conduct Code for ArchitectsDocument34 pagesProfessional Conduct Code for ArchitectsRiddhi PatelNo ratings yet
- Topic 8 Lawof Agency Part 1Document14 pagesTopic 8 Lawof Agency Part 1Zaid Chelsea100% (1)
- The Effect of Product Quality On Business Performance PDFDocument11 pagesThe Effect of Product Quality On Business Performance PDFSurajit SarbabidyaNo ratings yet
- Fair GlowDocument5 pagesFair GlowDeepali ChananaNo ratings yet
- Call Centre Investment ProposalDocument3 pagesCall Centre Investment ProposalPredueElleNo ratings yet
- S&D Group 1 Assignment CDocument9 pagesS&D Group 1 Assignment Cm omprakashNo ratings yet