You might also like
- EMQs For Medical Students Volume 3 2eDocument16 pagesEMQs For Medical Students Volume 3 2ePasTestBooks50% (2)
- Data Interpretation For Medical StudentsDocument42 pagesData Interpretation For Medical StudentsPasTestBooks100% (6)
- EMQs For Medical Students Volume 2 2eDocument30 pagesEMQs For Medical Students Volume 2 2ePasTestBooks50% (2)
- EMQs For Medical Students Volume 1 2EDocument27 pagesEMQs For Medical Students Volume 1 2EPasTestBooks100% (2)
- DIY Clinical Examination UG BOOKDocument20 pagesDIY Clinical Examination UG BOOKPasTestBooksNo ratings yet
- Oscesbook 1Document38 pagesOscesbook 1PasTestBooks100% (1)
- MRCPCH Part 1 Questions With Individual Subject Summaries 4eDocument52 pagesMRCPCH Part 1 Questions With Individual Subject Summaries 4ePasTestBooks88% (25)
- MRCPCH Clinical: Short Cases, History Taking & Communication Skills 3eDocument19 pagesMRCPCH Clinical: Short Cases, History Taking & Communication Skills 3ePasTestBooks100% (5)
- Ern MRCPCHDocument24 pagesErn MRCPCHPasTestBooksNo ratings yet
- MRCP ErnDocument41 pagesMRCP ErnPasTestBooksNo ratings yet
- MRCP ErnDocument41 pagesMRCP ErnPasTestBooksNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Tensiometro Cvs PharmacyDocument38 pagesTensiometro Cvs PharmacyAlfredo PonsNo ratings yet
- Using The Surface Electrocardiogram To Localization of Idiopathic Ventricular TachycardiaDocument12 pagesUsing The Surface Electrocardiogram To Localization of Idiopathic Ventricular TachycardiaNavojit ChowdhuryNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- Pathogenesis of Circulatory ShockDocument28 pagesPathogenesis of Circulatory ShockWan Razin Wan HassanNo ratings yet
- Cardio Vascular System NursingDocument2 pagesCardio Vascular System NursingGade BalajiNo ratings yet
- IsdnDocument5 pagesIsdnWidya JelitaNo ratings yet
- Clinical Trials in Cardiology 2nd Ed PDFDocument272 pagesClinical Trials in Cardiology 2nd Ed PDFIrving H Torres LopezNo ratings yet
- Cardiovascular DisordersDocument20 pagesCardiovascular DisordersHampson MalekanoNo ratings yet
- Cardiac CycleDocument2 pagesCardiac CycleU Than HanNo ratings yet
- Acute Atrial Fibrillation DavidsonDocument6 pagesAcute Atrial Fibrillation DavidsonAamir BugtiNo ratings yet
- Pulmonary EmbolismDocument3 pagesPulmonary EmbolismdeanneadrianoNo ratings yet
- Cardiovasular SystemDocument5 pagesCardiovasular SystemAsher Eby VargeeseNo ratings yet
- Cicrulatory and Immune Workbook KEYDocument32 pagesCicrulatory and Immune Workbook KEYgeorgia robinsonNo ratings yet
- Cardiovascular Management Using Yogic TechniquesDocument3 pagesCardiovascular Management Using Yogic TechniquesJacklynlim LkcNo ratings yet
- 2020 Focused Transesophageal Echocardiography During Cardiac Arrest ResuscitationDocument10 pages2020 Focused Transesophageal Echocardiography During Cardiac Arrest Resuscitationbogeg74816No ratings yet
- Brugada Syndrome: ECG Changes and Treatment OptionsDocument34 pagesBrugada Syndrome: ECG Changes and Treatment OptionsMohammad Irfan100% (1)
- PE's From Mark Hammerschmidt RN: WWW Icufaqs OrgDocument22 pagesPE's From Mark Hammerschmidt RN: WWW Icufaqs OrgMark Hammerschmidt50% (2)
- CPG Management of Percutaneous Coronory Intervention (PCI) 2009Document92 pagesCPG Management of Percutaneous Coronory Intervention (PCI) 2009umiraihana1No ratings yet
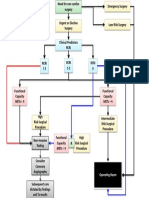
- Cardiac Risk Assessemnt FlowchartDocument1 pageCardiac Risk Assessemnt FlowchartjamesomooreNo ratings yet
- Noninvasive Monitoring 2016Document6 pagesNoninvasive Monitoring 2016Maria LaiaNo ratings yet
- PhysiologyDocument31 pagesPhysiologyraza20No ratings yet
- Kami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedDocument4 pagesKami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedKoleen Lhyte T. UYNo ratings yet
- Congenital Heart DiseaseDocument10 pagesCongenital Heart DiseaseIca JustitiaNo ratings yet
- Paxton V Cedars SACDocument42 pagesPaxton V Cedars SACTHROnlineNo ratings yet
- Anandhi ResumeDocument7 pagesAnandhi ResumeAnonymous rMa4DVY5J2No ratings yet
- Esmoe CTG 2022Document64 pagesEsmoe CTG 2022TangiNo ratings yet
- Ecg TestDocument67 pagesEcg TestEm KayNo ratings yet
- Excursion WorksheetDocument6 pagesExcursion Worksheetapi-348781812No ratings yet
- Introduction to Cardiac UltrasoundDocument26 pagesIntroduction to Cardiac UltrasoundSandra GutierrezNo ratings yet
- Electrocardiographic Monitoring 2017Document72 pagesElectrocardiographic Monitoring 2017Mirela Marina BlajNo ratings yet