You might also like
- Bowel Obstruction Surgery: Causes, Risks, and RecoveryDocument12 pagesBowel Obstruction Surgery: Causes, Risks, and RecoveryDivya JoyNo ratings yet
- Purpose: Billroth I, More Formally Billroth's Operation I, Is AnDocument8 pagesPurpose: Billroth I, More Formally Billroth's Operation I, Is AnttriggerNo ratings yet
- Management of Intestinal ObstructionDocument33 pagesManagement of Intestinal ObstructionSya Samat100% (1)
- CholecystectomyDocument5 pagesCholecystectomyRachelle Maderazo CartinNo ratings yet
- Acute Gallbladder InflammationDocument13 pagesAcute Gallbladder InflammationDivine Ballesteros Dela CruzNo ratings yet
- Blunt Abdominal InjuryDocument6 pagesBlunt Abdominal InjuryPeter KayNo ratings yet
- ER AnalysisDocument11 pagesER AnalysisReal TetisoraNo ratings yet
- Small & Large Intestines - LectureDocument70 pagesSmall & Large Intestines - Lecturehussain AltaherNo ratings yet
- Treatments and Drugs: by Mayo Clinic StaffDocument23 pagesTreatments and Drugs: by Mayo Clinic StaffJr D BayzNo ratings yet
- Choledocal CystDocument11 pagesCholedocal CystBilly JonatanNo ratings yet
- CHOLECYSTECTOMYDocument9 pagesCHOLECYSTECTOMYGuenever Tesoro100% (1)
- GistDocument5 pagesGistYip Kar JunNo ratings yet
- Chole SysDocument8 pagesChole SysKas MulyadiNo ratings yet
- Cholecystectomy and Nursing Care PlanDocument8 pagesCholecystectomy and Nursing Care PlanLara GatbontonNo ratings yet
- Abdominal Paracentesis Procedure GuideDocument14 pagesAbdominal Paracentesis Procedure Guideesther100% (1)
- Biliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou UniversityDocument42 pagesBiliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- BiliaryDocument41 pagesBiliaryayundyawibowoNo ratings yet
- Gastric Resection: General Surgical and Anesthetic ConsiderationsDocument26 pagesGastric Resection: General Surgical and Anesthetic ConsiderationsBlanchette ChNo ratings yet
- GASTRECTOMYDocument3 pagesGASTRECTOMYMaria Ydela MeradoresNo ratings yet
- Doc1 Obstractive JaundiceDocument7 pagesDoc1 Obstractive JaundiceZhy CaluzaNo ratings yet
- Bowel Obstruction - ppt1Document30 pagesBowel Obstruction - ppt1Elfrida Aulia100% (1)
- Cholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is TheDocument3 pagesCholecystectomy: Cholecystectomy (Pronounced / Kɒləsɪs Tɛktəmi/, Plural: Cholecystectomies) Is Thejosias_jorgio1No ratings yet
- Colostomy and The GallbladderDocument13 pagesColostomy and The GallbladderJustin Ahorro-DionisioNo ratings yet
- CancerDocument10 pagesCancercitidotnetNo ratings yet
- Surgical ManagementDocument6 pagesSurgical ManagementAlthea DetallaNo ratings yet
- Cholecystectomy 4 PrintingDocument19 pagesCholecystectomy 4 PrintingKyle Punzalan100% (2)
- Patient Guide to Appendectomy CareDocument9 pagesPatient Guide to Appendectomy CareJuan Sergio Tello ArroyoNo ratings yet
- DYSPHAGIADocument76 pagesDYSPHAGIASaurabh AgarwalNo ratings yet
- NCM112 LP1 Rosales - AnswersDocument5 pagesNCM112 LP1 Rosales - AnswersChristine CalleyNo ratings yet
- Subjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationDocument18 pagesSubjective: Goals: - : Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationJennalyn Padua SevillaNo ratings yet
- LOGBOOK MODULE 5 Blok 2.6Document20 pagesLOGBOOK MODULE 5 Blok 2.6nurbalqis204No ratings yet
- Open CholecystectomyDocument35 pagesOpen CholecystectomywqNo ratings yet
- Role of Radiology in Acute AbdomenDocument37 pagesRole of Radiology in Acute AbdomenAli TahirNo ratings yet
- Fistulas EnglishDocument19 pagesFistulas EnglishKarim AL-TijaniNo ratings yet
- Case Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyDocument46 pagesCase Study Presented by Group 22 BSN 206: In-Depth View On CholecystectomyAjiMary M. DomingoNo ratings yet
- Interventions For Patient With DiverticulosisDocument2 pagesInterventions For Patient With DiverticulosisImnot YouNo ratings yet
- San Pablo Colleges Medical Center case presentation on cholelithiasisDocument43 pagesSan Pablo Colleges Medical Center case presentation on cholelithiasisMary Rose LinatocNo ratings yet
- Laparoscopic Gastrointestinal SurgeryDocument22 pagesLaparoscopic Gastrointestinal SurgeryRoxana BoloagaNo ratings yet
- Intestinal Obstruction: Ahmed Badrek-AmoudiDocument26 pagesIntestinal Obstruction: Ahmed Badrek-Amoudiselvie87No ratings yet
- CHOLEDocument25 pagesCHOLEJane TuazonNo ratings yet
- Chapter VDocument15 pagesChapter VJellou MacNo ratings yet
- Abdominal US in Equine GI DiseaseDocument14 pagesAbdominal US in Equine GI Diseasedanielaayala6095No ratings yet
- Hepato-Biliary System 26.4.2016Document59 pagesHepato-Biliary System 26.4.2016S B SayedNo ratings yet
- Bowel ObstructionDocument10 pagesBowel Obstructionenke.nwekeNo ratings yet
- Diagnostic Liver Biopsy PDFDocument7 pagesDiagnostic Liver Biopsy PDFAriadna MarielNo ratings yet
- Liver Cirrhosis Case PresDocument77 pagesLiver Cirrhosis Case Presmarlx580% (5)
- Lectura 8Document8 pagesLectura 8Daniela Andrea Tello GuaguaNo ratings yet
- Rationale Diagnostic ProceduresDocument22 pagesRationale Diagnostic ProceduresShaktisila FatrahadyNo ratings yet
- Cancer Site Screening, Laboratory Test Diagnostic Test and Tumor Markers Nursing Responsibility in Preparing The Client and Significant OtherDocument9 pagesCancer Site Screening, Laboratory Test Diagnostic Test and Tumor Markers Nursing Responsibility in Preparing The Client and Significant OtherKei CruzNo ratings yet
- Jurding English FIXDocument24 pagesJurding English FIXDias Amardeka Putri GavintaNo ratings yet
- Small Bowel Emergency Surgery Literatures ReviewDocument6 pagesSmall Bowel Emergency Surgery Literatures Reviewc5pbp8dkNo ratings yet
- Ultrasound (U.S.G.) : IntroductionDocument4 pagesUltrasound (U.S.G.) : IntroductionAmit MartinNo ratings yet
- Complications of Ovariohysterectomy and Orchiectomy in Companion AnimalsDocument17 pagesComplications of Ovariohysterectomy and Orchiectomy in Companion AnimalsCarolina Soler GómezNo ratings yet
- CholecystectomyDocument5 pagesCholecystectomydkbjNo ratings yet
- AXR PresentationDocument30 pagesAXR PresentationLalit KumarNo ratings yet
- Trastornos Motores Esofagicos 2Document8 pagesTrastornos Motores Esofagicos 2Jose CarlosNo ratings yet
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Thyroid Encyclopedia: Encyclopedia of Thyroid Disease, Thyroid Conditions and Thyroid CancerFrom EverandThyroid Encyclopedia: Encyclopedia of Thyroid Disease, Thyroid Conditions and Thyroid CancerNo ratings yet
- Roman ArchitectureDocument166 pagesRoman ArchitectureKatherine 'Chingboo' Leonico Laud100% (4)
- Anatomy and Physiology:gastrointestinal Tract Powerpoint PresentationDocument28 pagesAnatomy and Physiology:gastrointestinal Tract Powerpoint PresentationKatherine 'Chingboo' Leonico Laud100% (15)
- Greek ArchitectureDocument107 pagesGreek ArchitectureKatherine 'Chingboo' Leonico Laud100% (1)
- CP Intestinal Obstruction PathoPhysiologyDocument4 pagesCP Intestinal Obstruction PathoPhysiologyKatherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction PrioritizationDocument2 pagesCP Intestinal Obstruction PrioritizationKatherine 'Chingboo' Leonico LaudNo ratings yet
- Sample Gordon's Functional Health Pattern: Intestinal ObstructionDocument23 pagesSample Gordon's Functional Health Pattern: Intestinal ObstructionKatherine 'Chingboo' Leonico Laud93% (28)
- CP Intestinal Obstruction PrognosisDocument2 pagesCP Intestinal Obstruction PrognosisKatherine 'Chingboo' Leonico Laud100% (1)
- CP Intestinal Obstruction Intestinal ObstructionDocument126 pagesCP Intestinal Obstruction Intestinal ObstructionKatherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Chap4Document17 pagesCP Intestinal Obstruction Chap4Katherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Drug StudyDocument26 pagesCP Intestinal Obstruction Drug StudyKatherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Nursing Care PlanDocument7 pagesCP Intestinal Obstruction Nursing Care PlanKatherine 'Chingboo' Leonico Laud95% (20)
- CP Intestinal Obstruction Chap5Document23 pagesCP Intestinal Obstruction Chap5Katherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Nursing Care PlanDocument7 pagesCP Intestinal Obstruction Nursing Care PlanKatherine 'Chingboo' Leonico Laud95% (20)
- CP Intestinal Obstruction Title PageDocument6 pagesCP Intestinal Obstruction Title PageKatherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Chap8Document18 pagesCP Intestinal Obstruction Chap8Katherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Title PageDocument1 pageCrisis Intervention: Psychiatric Nursing Title PageKatherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction PathoPhysiologyDocument4 pagesCP Intestinal Obstruction PathoPhysiologyKatherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Chap3Document1 pageCP Intestinal Obstruction Chap3Katherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Chap9Document1 pageCrisis Intervention: Psychiatric Nursing Chap9Katherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Chap2Document2 pagesCP Intestinal Obstruction Chap2Katherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Chap1Document3 pagesCP Intestinal Obstruction Chap1Katherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Chap7Document2 pagesCrisis Intervention: Psychiatric Nursing Chap7Katherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Chap11Document2 pagesCrisis Intervention: Psychiatric Nursing Chap11Katherine 'Chingboo' Leonico LaudNo ratings yet
- CP Intestinal Obstruction Bibliography VitaeDocument5 pagesCP Intestinal Obstruction Bibliography VitaeKatherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Table of ContentsDocument1 pageCrisis Intervention: Psychiatric Nursing Table of ContentsKatherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Nursing Care PlanDocument13 pagesCrisis Intervention: Psychiatric Nursing Nursing Care PlanKatherine 'Chingboo' Leonico Laud100% (4)
- Crisis Intervention: Psychiatric Nursing Chap10Document7 pagesCrisis Intervention: Psychiatric Nursing Chap10Katherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Chap6Document7 pagesCrisis Intervention: Psychiatric Nursing Chap6Katherine 'Chingboo' Leonico LaudNo ratings yet
- Crisis Intervention: Psychiatric Nursing Chap8Document17 pagesCrisis Intervention: Psychiatric Nursing Chap8Katherine 'Chingboo' Leonico LaudNo ratings yet
- Auditory Brainstem Response - ABR - in Clinical Practice PDFDocument9 pagesAuditory Brainstem Response - ABR - in Clinical Practice PDFary wisma dewiNo ratings yet
- QuestionsDocument6 pagesQuestionsLorvic Andrew Juanson UmaliNo ratings yet
- Advances in Extraction TechniquesDocument13 pagesAdvances in Extraction TechniquesashajangamNo ratings yet
- Presented By: Meljyn Gomez Cuyos Dy, Arvie Jane Ederango, Nemia Bless Marjory, Epe Aizyl, FloresDocument32 pagesPresented By: Meljyn Gomez Cuyos Dy, Arvie Jane Ederango, Nemia Bless Marjory, Epe Aizyl, FloresJuviely PremacioNo ratings yet
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNo ratings yet
- 7-Physiology of Normal PuerperiumDocument24 pages7-Physiology of Normal Puerperiumhade elNo ratings yet
- A Case of Beauvieux'S Syndrome and Its EvolutionDocument7 pagesA Case of Beauvieux'S Syndrome and Its EvolutionAndrea ModestieNo ratings yet
- Case Study PneumothoraxDocument9 pagesCase Study PneumothoraxLee_Cabral_693967% (3)
- Rheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009Document9 pagesRheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009drwstokes100% (1)
- Windkessel EffectDocument11 pagesWindkessel EffectAkhmad HidayatNo ratings yet
- Chapter 15 - Hormones & Endocrine GlandsDocument17 pagesChapter 15 - Hormones & Endocrine Glandsapi-3728508100% (1)
- Multiple PregnancyDocument16 pagesMultiple Pregnancyjane7arian7berzabalNo ratings yet
- BLEPHAROKERATOCONJUNCTIVITIS: EYE INFLAMMATIONDocument15 pagesBLEPHAROKERATOCONJUNCTIVITIS: EYE INFLAMMATIONWaiwit KritayakiranaNo ratings yet
- 2022 Book AntimicrobialResistanceDocument606 pages2022 Book AntimicrobialResistanceFety Andriani100% (1)
- Diabetes Care GuideDocument14 pagesDiabetes Care GuideadaezeNo ratings yet
- Ann JeinaDocument7 pagesAnn JeinaMizumoriFumairaNo ratings yet
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- Important Classifications PDFDocument42 pagesImportant Classifications PDF330 Himank MehtaNo ratings yet
- Autism Facts vs Myths: Debunking Common MisconceptionsDocument14 pagesAutism Facts vs Myths: Debunking Common Misconceptionsawardeco01No ratings yet
- Minimum Inhibitory ConcentrationDocument7 pagesMinimum Inhibitory ConcentrationToshio HamazakiNo ratings yet
- Theory and Practice of Pure Tone Audiometry - PTADocument12 pagesTheory and Practice of Pure Tone Audiometry - PTAsolhazNo ratings yet
- Basic pharmacology of anaesthesia drugs in 40 charactersDocument56 pagesBasic pharmacology of anaesthesia drugs in 40 charactersrajvikram87No ratings yet
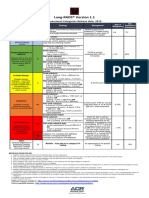
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Femoral Acetabular Impingement: RadiographyDocument9 pagesFemoral Acetabular Impingement: Radiography杨钦杰No ratings yet
- Cpdprogram Nursing 81718Document301 pagesCpdprogram Nursing 81718PRC BoardNo ratings yet
- Neonatal Emergencies FinalDocument90 pagesNeonatal Emergencies FinalDr Raseena VattamkandathilNo ratings yet
- Psoriasis and Miracles With HomoeopathyDocument3 pagesPsoriasis and Miracles With HomoeopathyEditor IJTSRDNo ratings yet
- GROUP 10 Senstive Abt Food and Food AllergiesDocument16 pagesGROUP 10 Senstive Abt Food and Food AllergiesLilis nopita SarryNo ratings yet
- Eric Berg CVDocument6 pagesEric Berg CVHaralambicNo ratings yet
- Medical EmergencyDocument2 pagesMedical EmergencyPrashant MathuriaNo ratings yet