You might also like
- Acupressure Be Your Own DoctorDocument69 pagesAcupressure Be Your Own DoctorGanesan Murusamy100% (1)
- Rare Collections SignaturesDocument17 pagesRare Collections SignaturesnandhumangoNo ratings yet
- Oral Motor ExercisesDocument5 pagesOral Motor ExercisesMayzatt MaisyaNo ratings yet
- Mathematical Entertainments - A Collection of Illuminating Puzzles, New and OldDocument173 pagesMathematical Entertainments - A Collection of Illuminating Puzzles, New and OldsheetalparshadNo ratings yet
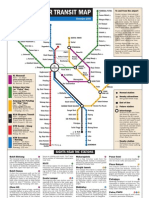
- KL Transit MapDocument1 pageKL Transit MapWong PfNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Measles/ Rubella & VPD Surveillance:: Allotment of EPID Number and Outbreak IDDocument7 pagesMeasles/ Rubella & VPD Surveillance:: Allotment of EPID Number and Outbreak IDDevendra Singh TomarNo ratings yet
- MicrosystemDocument5 pagesMicrosystembabalalaNo ratings yet
- Arthropods: A Guide to the Diverse PhylumDocument10 pagesArthropods: A Guide to the Diverse Phylumpkkalai112No ratings yet
- Theoretical Framework for Measuring Job Satisfaction (SampleDocument4 pagesTheoretical Framework for Measuring Job Satisfaction (SampleJoseEdgarNolascoLucesNo ratings yet
- Global Chlor - Alkali Market Statistics Update June 16 2014Document31 pagesGlobal Chlor - Alkali Market Statistics Update June 16 2014diego_cáceres_30No ratings yet
- Project Report On Biodegradable Plates, Glasses, Food Container, Spoon Etc.Document6 pagesProject Report On Biodegradable Plates, Glasses, Food Container, Spoon Etc.EIRI Board of Consultants and Publishers0% (1)
- 4front Projects: BbbeeDocument12 pages4front Projects: BbbeeBrand Media OfficeNo ratings yet
- Behavior Intervention PlanDocument6 pagesBehavior Intervention Planapi-308475283No ratings yet
- 23soft Starter HandbookDocument36 pages23soft Starter HandbookCarlos_Duque1958No ratings yet
- Structure Dismantling JSADocument2 pagesStructure Dismantling JSAtnssbhaskar69% (13)
- Auxiliary Range: CLR - High Speed Trip Lockout RelayDocument2 pagesAuxiliary Range: CLR - High Speed Trip Lockout Relaydave chaudhuryNo ratings yet
- Worksheet - Solubility - Water As A SolventDocument2 pagesWorksheet - Solubility - Water As A Solventben4657No ratings yet
- FAQ: Product RegistrationDocument5 pagesFAQ: Product RegistrationCalvin WangNo ratings yet
- Atlas Copco Generators: 15-360 kVA 15-300 KWDocument10 pagesAtlas Copco Generators: 15-360 kVA 15-300 KWAyoub SolhiNo ratings yet
- Installation TubeeeDocument7 pagesInstallation TubeeeDini NovitrianingsihNo ratings yet
- MIDWIFE1115ra Tugue e PDFDocument9 pagesMIDWIFE1115ra Tugue e PDFPhilBoardResultsNo ratings yet
- Employment Law Lubs 3915Document4 pagesEmployment Law Lubs 3915ogunsatoNo ratings yet
- Science 6-Q1-M6Document14 pagesScience 6-Q1-M6John Philip LegaspiNo ratings yet
- NCM 117 Rle NAME: Guerzo, Danniel Dave Y. DATE/TIME: March 9, 2023 Section/Year Level: BSN 3B Group No:10 CIDocument2 pagesNCM 117 Rle NAME: Guerzo, Danniel Dave Y. DATE/TIME: March 9, 2023 Section/Year Level: BSN 3B Group No:10 CISherlyn Miranda GarcesNo ratings yet
- BrochureDocument2 pagesBrochureRajib DasNo ratings yet
- AMGG-S - 1 - Environmental Safeguard Monitoring - 25.03.2021Document48 pagesAMGG-S - 1 - Environmental Safeguard Monitoring - 25.03.2021Mahidul Islam RatulNo ratings yet
- Environmental Stewardship - Sustainability Assignment - Ethan GabrielDocument3 pagesEnvironmental Stewardship - Sustainability Assignment - Ethan GabrielEthan GabrielNo ratings yet
- Mitsubishi v500 VFD IB NA 0600065-F FR-V500-NA Instruction Manual-DetailedDocument221 pagesMitsubishi v500 VFD IB NA 0600065-F FR-V500-NA Instruction Manual-DetailedMROstop.comNo ratings yet
- Binac Ao STR EET: Vicinity Map & Street View, Source Google MapsDocument17 pagesBinac Ao STR EET: Vicinity Map & Street View, Source Google MapsBee AnquilianoNo ratings yet
- 2022 Intro To Process and Plant Safety NewDocument163 pages2022 Intro To Process and Plant Safety Newdavid gabriel100% (2)
- My PRC Form-Censored Case NumbersDocument5 pagesMy PRC Form-Censored Case NumbersLeah Lou Gerona MontesclarosNo ratings yet
- Dladla Effect 2013Document231 pagesDladla Effect 2013TheDreamMNo ratings yet
- Knorr FinalDocument25 pagesKnorr Finalimbree100% (3)
- Louise L HAY AffirmationsDocument10 pagesLouise L HAY AffirmationsEvi Kutasi100% (2)
- Greek God and Goddess ListDocument3 pagesGreek God and Goddess Listapi-359276609No ratings yet