Professional Documents
Culture Documents
Biomechanics and Physiology in Active Manual Wheelchair Propulsion
Uploaded by
Stanislas AchardOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Biomechanics and Physiology in Active Manual Wheelchair Propulsion
Uploaded by
Stanislas AchardCopyright:
Available Formats
Medical Engineering & Physics 23 (2001) 713733 www.elsevier.
com/locate/medengphy
Biomechanics and physiology in active manual wheelchair propulsion1
L.H.V. van der Woude a,*, H.E.J. Veeger a, b, A.J. Dallmeijer a, T.W.J. Janssen a, c, L.A. Rozendaal a
a
Institute for Fundamental and Clinical Human Movement Science, Faculty of Human Movement Sciences, Vrije Universiteit, Van der Boechorststraat 9, 1081 BT Amsterdam, The Netherlands b Man Machine Systems, Delft University of Technology, Delft, The Netherlands c Rehabilitation Center Amsterdam, The Netherlands Received 19 July 2001; accepted 10 August 2001
Abstract Manual wheelchair propulsion in daily life and sports is increasingly being studied. Initially, an engineering and physiological perspective was taken. More recently a concomitant biomechanics interest is seen. Themes of biomechanical and physiological studies today are performance enhancing aspects of wheelchair use and the ergonomics of wheelchair design. Apart from the propulsion technique the focus of biomechanics research of manual wheelchair propulsion is mainly towards injury mechanisms, especially phenomena of overuse to the upper extremity. Obviously, the vehicle mechanics of wheelchairs must be included within this biological framework. Scientic research is progressing, but is still hampered by methodological limitations, such as the heterogeneity and small numbers of the population at study as well as the inconsistency of employed technologies and methodologies. There is a need for consensus regarding methodology and research strategy, and a strong need for collaboration to improve the homogeneity and size of subject groups and thus the power of the experimental results. Thus a sufciently strong knowledge database will emerge, leading to an evidence-base of performance enhancing factors and the understanding of the risks of wheelchair sports and long-term wheelchair use. In the light of the current biomechanical and physiological knowledge of manual wheelchair propulsion there seems to be a need for the stimulation of other than hand rim propelled manual wheelchairs. 2002 IPEM. Published by Elsevier Science Ltd. All rights reserved.
Keywords: Biomechanics; Physiology; Modeling; Performance capacity; Wheelchair propulsion technique; Vehicle mechanics; Interface
1. Introduction Over the years, hand rim wheelchairs have changed from chromium-plated wheelchairs for daily use in the early sixties to the current high-tech and task specic devices. These wheelchairs are commonly tuned to individual characteristics. During the last few decades researchers have contributed considerably to the understanding of wheelchair arm work in daily life and wheelchair sports performance [2]. Research initially
* Corresponding author. Tel.: +31-20-4448500; fax: +31-204448529. E-mail address: lvdwoude@fbw.vu.nl (L.H.V. van der Woude). 1 In adapted form, published as Woude et al. [1].
started much more from a mechanical point of view, focusing on materials, durability, safety and vehicle mechanics [310]. Despite a start in the late sixties [11,12], at a much later stage interest in manual wheelchair propulsion was directed towards the physiological and health related consequences. Even more recently, attention was more consistently also geared towards the biomechanical aspects of wheelchair propulsion [1324]. A detailed engineering perspective of different aspects of wheeled mobility is given by Cooper [25]. Initially, biomechanics and physiology focused towards performance related issues with relatively simple technology and methodology. Despite the major improvement in technology, propulsion technique is still
1350-4533/02/$22.00 2002 IPEM. Published by Elsevier Science Ltd. All rights reserved. PII: S 1 3 5 0 - 4 5 3 3 ( 0 1 ) 0 0 0 8 3 - 2
714
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
not very well understood today. More recently, biomechanics research has been geared towards the musculoskeletal problems of long-term wheelchair use and sports. Today, within the framework of active wheelchair use, a number of relevant research questions can be categorized. There are a number of performance associated issues: propulsion technique, (peak) power production, short-term peak power or anaerobic power production. But also disability related issues must be raised, for instance with respect to questions directly associated with the human stressstraincapacity problem. Obviously, research questions may also address the ergonomics of wheelchair design and tting. Three basic qualities of the wheelchairuser combination determine the nal performance in wheelchair use [26]: (1) the user the motor who essentially produces the energy and power for propulsion; (2) the technical status and vehicle mechanics of the wheelchair itself which determine the power requirements; (3) the wheelchairuser interaction which essentially will determine the efciency of power transfer from the motor to the wheelchair. The contribution of biomechanics and physiology to the understanding of these three elements and in attaining and improving maximum performance in wheelchair sports and daily use will be exemplied below. Obviously, a wide variety of hand propelled wheelchairs is available on the market. One cannot speak of the wheelchair, even if we isolate the hand rim propelled wheelchair, which is predominantly used in daily life and sports. Even small variations in wheelchair conguration will lead to differences in the manmachine interaction and in vehicle mechanics. This will subsequently inuence physiological and biomechanical measures of performance. Only recently, the advantages of crank and lever propelled wheelchairs (tricycles) have become evident to the athletes and wheelchair users in general. Today the handcycle or handbike propulsion mechanisms are becoming increasingly popular and are used in recreation, outdoors and in an increasing number of open competitions and events [2729]. Given the dominance of hand rim propulsion, the emphasis in this paper will primarily be on the hand rim interface type.
of work (A). The advantage of this approach is that physiological measures (i.e. energy cost, physical strain) can elegantly be linked with biomechanical measures (i.e. power output, work, force and torque production). The product of push frequency (f) and work (A) gives the average external power output (Po), according to: Po fA (W) (1)
The work produced in each push constitutes the integral of the momentary torque (M) applied by the hands to the hand rim over a more or less xed angular displacement (Q). In hand rim propulsion, the push is discontinuous, under steady state conditions highly reproducible, and generally is limited to an angle of 7080 [32], given the constraints of the sitting posture, functional anatomy of the upper body and the spatial orientation of the rim. In wheelchair track sports, basically other propulsion techniques are employed [33,34]. These will not be addressed in detail here. The above equation can be rewritten into: Po f MdQ (W) (2)
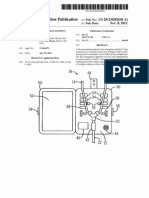
where torque is the product of the bi-manual tangential force, which is applied on the hand rim, and the radius of the hand rim. Measurement of angular displacement and the torque around the wheel-axle requires specialized experimental techniques for motion analysis and force measurement, which are not widely available. Therefore, a different approach to determining Po is frequently employed. Here the forces resisting the wheelchairuser combination are taken as the starting point for the calculation of power output. The wheelchairuser combination is approached as a free body that moves at a given speed (v) and encounters the following (drag) forces: rolling friction (Froll), air resistance (Fair), gravitational effects when going up/down a slope (mg sin a) and internal friction (Fint). Details of these forces will be discussed below. The product of the sum of these drag forces (Fdrag) and the linear velocity of the free body equals the power output that must be produced to maintain that velocity, according to: Po Fdragv (W) (3)
2. Research strategy 2.1. Cyclic movement Manual wheelchair propulsion is frequently studied as a cyclic movement pattern [26,30,31]; a given propelling motion is repeated over time at a given frequency (f), generally to maintain a certain stationary velocity (v). This implies that in each stroke or push of the wheel the wheelchairuser produces a more or less equal amount
The drag force can fairly easily be determined through a drag test [31,35] (Fig. 1). 2.2. Arm work and gross mechanical efciency Power production during wheelchair propulsion is achieved by upper body work, primarily the arms. The relatively small muscle mass of the upper extremities and increased tendency for local fatigue leads to a much lower maximal work capacity in comparison to legwork. Peak oxygen uptake is usually 6085% of that in leg-
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
715
work [36]. Measurement of power output in wheelchair exercise testing, in combination with physiological measurements of the cardio-respiratory strain, gives additional information on the physical capacity of the person, and is also required for the calculation of the efciency of the wheelchairuser system. The gross mechanical efciency (ME) is dened as the ratio between externally produced energy (power out) and internally liberated energy (En: i.e. oxygen cost under submaximal, physiological steady state conditions), according to: ME (PoEn1)100 (%) (4)
The mechanical efciency of wheelchair propulsion is predominantly available from non-wheelchair users and is as low as 210% [31,32,3740], which is lower than in arm crank ergometry, where values of around 15% are commonly found [41]. To date, data on handbike use in wheelchair user populations are still only rarely available [28,42]. The gures for ME appear higher than those in hand rim propulsion (up to 1112%, as given by [31]), but no recent comparative studies on ME were made to our knowledge. The low efciency of hand rim wheelchair propulsion may be explained by the small muscle mass in comparison with legwork, the complex movement pattern and coupling technique to the rim, and the complex functional anatomy of the upper extremity. The mechanical efciency is highly inuenced by propulsion conditions, like (hand rim) velocity and resistance; efciency for instance increases with lower velocities and higher workload [32,40]. The conguration of the wheelchair, such as propulsion mechanism, seat height, and differences in individual propelling technique can also affect the mechanical efciency [26,32,37,40,4345]. 2.3. Experimental set-ups Specic and standardized laboratory experiments are required to analyze performance capacity in wheelchair users. Often this is customized equipment, which varies in reliability and validity. Obviously, the choice of experimental set-up is dependent on the research purpose, but also on the availability of measurement systems. Wheelchair tests are generally performed to investigate physical capacity of wheelchair users, to analyze wheelchair propulsion technique, to assess different wheelchair designs, or to evaluate load on the upper extremity joints. The least standardized but most realistic testing condition is a simple wheelchair (racing) track [4649]. Evidently, it is complicated to control experimental conditions and procedures, such as velocity and power output. This reduces reliability. Since the wheelchair user combination is non-stationary, physiological measures and kinematics are complicated to measure, but can
be accomplished with the currently available ambulant physiological and biomechanical measurement systems. Clearly, the validity of a wheelchair track is high and it may be a useful set-up to investigate biomechanics in combination with an instrumented wheelchair wheel that allows 3D force measurements [1719,21,5054]. The major advantage of an instrumented wheel will be the analysis of daily activities and wheelchair related tasks that cannot be met with stationary ergometry technology. Second best in terms of validity of wheelchair exercise testing is a motor driven treadmill. This device is widely used for research purposes. It allows valid physiological exercise testing, and the study of kinematics and muscle activity (a.o. [14,31,38,55]). Power output can be determined in the form of a simple drag test, in which the drag force of a wheelchairuser system can be determined [31,35] (Fig. 1). Workload can be varied with an inclination of the belt, or by applying a resistance force on the back of the wheelchair by means of a pulley system [38]. Calculation of power output from drag force and velocity enables the evaluation of efciency parameters for a given wheelchair system or conguration at submaximal, steady state exercise conditions. Variations in calculated drag force are generally small but may due to oscillations of the trunk, arms and head and the consequent effect on rolling friction increase up to 10% (non-published data). Treadmill wheelchair propulsion is mechanically realistic [30], showing a natural form of wheelchair propulsion with additional small steering corrections while rolling friction and inertia are realistic. Absence of air drag improves standardization, however it reduces validity, and probably has an (unstudied) effect on performance and propulsion technique. The treadmill set-up and track require the use of an actual (individual) wheelchair. This has advantages the wheelchairuser combination is highly trained. A disadvantage of using an actual wheelchair is that different wheelchair tting congurations is not easily done. Many different wheelchair ergometers have been developed, either with or without the actual use of a
Fig. 1.
Wheelchair dragtest on a motor driven treadmill.
716
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
wheelchair, sometimes linked to an existing (cycle) ergometer, or based on a roller system (a.o. [5660]). These set-ups use mechanical or electric brakes for resistance. Inertia is not always known, which limits the evaluation of realistic wheelchair propulsion characteristics. There are however roller based wheelchair ergometer systems that simulate actual wheeling accurately [45,61,62]. Since testing conditions are highly reproducible, this type of wheelchair ergometers are adequate for reliable exercise testing and evaluation of physical work capacity, in particular if the system can accurately measure external power. The nal category of wheelchair ergometers is the wheelchair simulator. Most of them are computer-controlled devices that accurately simulate wheelchair propulsion with an adjustable propulsion mechanism and/or seat conguration. Essentially it comes down to the simulation of wheelchair propulsion in terms of friction (rolling resistance, and sometimes air friction) and slope, and simulation of inertia of the wheelchairuser system. Most systems enable measurement of momentary torque and velocity, and thus power output [13,59,6367], and sometimes the measurement of 3D forces applied by the hand on the propulsion system [59,64,68]. Power, torque and force acquisition and analysis enable rather detailed studies of propulsion technique in conjunction with different standard physiological measures while the system does allow careful standardization of the wheelchair user conguration. In combination with 3D kinematic input, 3D force data can be used for biomechanical modeling. This can provide information on forces acting on the joints of the upper extremity [17,39,52,6974]. Modeling results will contribute to the understanding of the high incidence of musculo-skeletal disorders in wheelchair users and athletes [71,72,75]. With the growing interest in the biomechanics of manual wheelchair propulsion, the knowledge base of measurement technology, accuracy and validity grew [62,69,76,103], as well as the discussion on data interpretation, such as for instance the issue of the point of force application [17,53,77]. 2.4. Concluding remarks Diversity of measurement technology and methodology in biomechanical and physiological studies is in itself a problem. The comparability of results and of the applicability of the existing knowledge base is limited. There is a strong need for standardization and consensus with respect to applied measurement strategies, technologies and methodology. This is especially important in rehabilitation and in the eld of disabled sports, where small number studies and large inter-individual variations are inherently limiting the applicability of results and are a common issue of debate in this research eld.
3. Physical capacity The study of wheelchair propulsion is not only hampered by the large variety in research methods (see above), but also by the strong variability in functionality among studied subject groups. To initially overcome the inherent problem of the large heterogeneity of the disabled population, it seems quite appropriate to study non-wheelchair users rst, since they will be equally well (un-)trained on all tested conditions and obviously will physically be quite homogeneous. In the evaluation of design aspects of wheelchairs, such as propulsion mechanisms [26], or phenomena of learning [78], this seems a useful initial strategy. The effects of wheelchair arm work on the intact cardio-vascular and/or musculoskeletal systems can thus be quantied rst. Evidently, the consequence of disability on performance can subsequently be more accurately interpreted. Large number studies among wheelchair users have been limited, but are fortunately increasing in number [66,7984]. Various aerobic and anaerobic tests have been described, but little standardization is seen. In general, the ndings appear more or less consistent, but may be rather susceptible to the specics of the testing protocol. Most frequently, groups of athletes were studied [48,55,82,85]. A limited number of studies are available on sedentary wheelchair users [83], with predominance for subjects with a spinal cord injury [86], while groups of elderly subjects and children have hardly been studied [56,87,88]. Also, measurements usually focused on male subjects. For obvious reasons classication of subjects is a major issue in wheelchair sports and subject to strong debate. An optimal system of functional classication is however a prerequisite for fair competition. Studies such as that performed by Higgs et al. [89] have led to a reduction in the number of classes in the classication system of the International Stoke Mandiville Games Federation (ISMGF), and nally led to the introduction of a useful functional classication system. A further analysis of the fairness of classication systems requires systematic large number studies, or at least small number studies that are comparable to a high degree. What one needs to realize is however that individuals are different due to their inherent set of athletic qualities and talent apart from the level of disability that makes one athlete different from the other. To what extent disability is of inuence on performance capacity is again dependent on large number (longitudinal) studies. Results stress the strong variability among the wheelchair (athlete) population (see Table 1). 3.1. Aerobic capacity Tables 1 and 2 show the results of studies in which peak cardio-respiratory responses as well as power out-
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
717
Table 1 Aerobic capacity in male wheelchair athletes and sedentary subjects of some selected arm crank and wheelchair ergometry studiesa Authors Mode N ISMGF Disability VO2 (l min 1) VO2 (ml kg min 1) 40.6 32.9 27.3 23.0 26.8 36.9 40.6 39.4 27.1 40.6 23.9 34.5 23.9 14.6 Heart rate (b min 1) Power output (W)
Gass and Camp [55] Wicks et al. [80] Davis and Shephard [127] Veeger et al. [82]
MDT MDT ACE MDT
Gass et al. [128] Vinet et al. [129] Pare and Simard [66], sedentary Huonker et al. [81], athletes Huonker et al. [81], sedentary Keyser et al. [59] Woude et al. [42]
MDT WCE WCE WCE WCE WCE WCE
8 40 15 9 1 6 10 13 7 3 10 8 35 29 20 15 3 4 8 23
IcV IIIV Ic II III IV V Other IIIIV IIV T1 T2 T3 T4
T4L3 C7S1 T6L5 T4T6 C7C8 T1T5 T6T10 T11L3 L4S1 POL T8L3 T1 T1S2 SB, T2T12 a.o. SB, T2T12 C5/6C7 C7 T5L1 T6S1, POL, SB
2.23 2.24 1.72 1.64 1.84 1.97 2.42 2.38 2.94 1.94 2.67 1.63 1.76 1.14 1.14 0.67 1.30 2.04 2.29
175 182 177 150 170 175 182 182 160 181 174 187 183 162 146 110 133 183 187
81.1 97
66 80 85 79 93
39 89 50 22 51 86 106
a ACE: arm crank exercise; MDT: motor driven treadmill; WCE: wheelchair ergometry; T1 t/m T4: ISMGF functional classication; AMP: amputees; CP: cerebral palsy; HEM: hemiplegia; KA: knee artrodesis; POL: polio; SB: spina bida; SCI: spinal cord injury; F: female.
Table 2 Aerobic capacity in female wheelchair athletes and sedentary subjects of some selected wheelchair ergometry studiesa Authors Mode N ISMGF Disability VO2 (l min 1) VO2 (ml kg min 1) 20.7 25.5 33.9 36.1 38.6 33.7 18.3 Heart rate (b min 1) Power output (W)
Veeger et al. [82]
MDT
Vanlandewijck et al. [130], basketball
MDT
1 7 8 10 11 4 9 4 3 3 5 13 10
Ic IIIV All (Ic, IIIV) I (bas) II (bas) III (bas) IV (bas) T2 T3 T4 IIV (bas) IIII (bas)
C7/8 T6S1 C7/8S1 T3T12 T9T12 L1L5 AMP, POL, SB C5C7, POL T8, SB T12S1, SB, POL T1L5 T1L5
0.80 1.28 1.22 1.67 2.4 2.49 2.62 0.74 1.30 1.15 1.51 1.90 1.09
172 143 184 187 164 181 180
39 64 87 91 102 30 64 61 57 60 45
Woude et al. [29]
WCE
Schmid [131], athletes Schmid [131], sedentary
a
WCE WCE
MDT: motor driven treadmill; WCE: wheelchair ergometry; T1 t/m T4: ISMGF functional classication; bas: basketball; AMP: amputees; CP: cerebral palsy; HEM: hemiplegia; KA: knee artrodesis; POL: polio; SB: spina bida.
put were determined in male and female wheelchair athletes and sedentary subjects. Dependent on disability, values for maximal power output vary on average from around 20 W for persons with a cervical spinal cord injury or cerebral palsy, to around 100 W for persons with less severe disabilities (athletes with low paraplegia and amputees). For peak oxygen uptake mean values ranging from less than 1 l min 1 to a little less than
3 l min 1 are reported (Table 1). Physical capacity is considerably lower in females (Table 2). Variations in power output can also be inuenced by the used mode of exercise testing. Arm cranking is a widely used testing mode for persons with disabilities. However, because of the higher gross mechanical efciency in comparison with wheelchair ergometry higher peak power outputs are found in arm cranking
718
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
tests, whereas peak oxygen consumption is not substantially different. Therefore, when the interest is focused on hand rim wheelchair performance, wheelchair exercise testing is preferred over arm crank exercise testing. 3.2. Anaerobic capacity Values for anaerobic or sprint power (Table 3) again do show considerable inter-study variation, which is not solely the consequence of population variation, but is also inuenced by the used experimental setup and protocol [90]. In general, the sprint power output is calculated over a 30 s all-out sprinting test, indicative for anaerobic power output. Sprint performance is highly dependent on the resistance subjects are exposed to; Veeger et al. [90] showed decreases in mean sprint power output as a consequence of a lower resistance. This decline is the consequence of a higher mean linear hand velocity (in the push phase) with a lower resistance. Again, in arm cranking higher maximal power outputs are found in comparison with wheelchair arm work. Mean anaerobic power production in the wheelchair sprint test did not exceed 200 W. As a consequence of disability, extremely low values for power output were seen in subjects with cerebral palsy or with a cervical spinal cord injury.
3.3. Concluding remarks Apart from standardized testing procedures large number studies help to increase the power of the knowledge base. International collaboration and consensus regarding methodology are required to establish the determining inuence of training, functional ability and technique on performance, tness and health related issues. In order to set exercise and training goals there is a need for normative wheelchair arm work databases with (sub-)group performance limits, ordered according to functionality criteria (i.e. classication; age; training status). Systematic and detailed analyses of large number studies available today can help to generate evidencebased doseresponse relationships (for work capacity, tness, health) and thus generate training guidelines.
4. Biomechanics of wheelchair propulsion Over the last decade, manual wheelchair propulsion and wheelchair sports have increasingly become the subject of detailed biomechanical analyses. The current main reason for the strong biomechanics interest in wheelchair propulsion is apart from the study of performance the high mechanical loads on the upper
Table 3 Sprint power production in wheelchair athletes and sedentary subjects (men and women) for a number of studiesa Authors Modus N ISMGF Disability Peak sprint Po (W) 46 143 85 102149b 41.4 70.4 95.9 114.4 100.5 23 68 100 138 35 121 38 77 76 280 336 443 394 341 Peak sprint Po (W kg 1) 0.77 2.02 1.73 0.51 0.85 1.22 1.45 1.47 0.36 1.03 1.65 2.36 0.51 1.85 0.83 1.47 1.51
Coutts and Stogryn [132]
WCE
Lees and Arthur [133] Janssen et al. [83], sedentary
WCE WCE
Woude et al. [84]
WCE
Hutzler et al. [134]
ACE
2 3 1 (F) 6 9 6 15 12 2 3 4 8 23 6 (1F) 6 (1F) 4 (F) 3 (F) 3 (F) 13 15 10 12 40
Ia, Ib IIIV IV IIV I II III IV V T1 T2 T3 T4
C6C7 T9T12, POL T10 T1L5
T2 T3 T4 II IIIVI AMP POL All
C5/6C7 C7 T5L1 T6S1, POL, SB CP AMP, KA, HEM C5C7, POL T8, SB T12S1, SB, POL T1T5 T6S5 AMP POL
ACE: armcrank ergometry; WCE: wheelchair ergometry; T1 t/m T4: ISMGF functional classication; AMP: amputees; CP: cerebral palsy; HEM: hemiplegia; KA: knee artrodesis; POL: polio; SB: spina bida; F: female. b Values in dependence of different workloads.
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
719
extremity. These often lead to overload injuries in the wrist and lower arm and in the shoulder [71,72,75,91 95]. To gain insight in the causes and consequences of these high loads, as well as to study propulsion technique as such, biomechanical analysis is a prerequisite. Of course, the propulsion technique is highly dependent on the type of wheelchair used, as well as the functional capacity of the user. As a consequence, direct application of most of the ndings is rather difcult. It should be kept in mind, that almost all available kinetic information is based on studies focusing on daily use, tennis or basketball low velocity hand rim wheelchair propulsion. As a consequence, little will be said about athletic propulsion techniques, such as the buttery technique. These (buttery like) beating techniques deviate considerably from the more general grabbing technique and have been studied to a limited extent [33,34,85,96]. The mechanical stress on the musculoskeletal system is high in hand rim wheelchair propulsion. As a consequence, shoulder pain, as well as carpal tunnel syndrome, are common problems for wheelchair athletes and users in general [71,72,93,97,98]. The high mechanical load on the upper extremity in hand rim wheelchair propulsion can, within the framework of the task (repetitious, peak force, limited muscle use, extreme joint deections (wrist)), at least partially be explained from the complex anatomy of arm and shoulder. More specically, the complaints might be related to the necessity to stabilize the glenohumeral (GH) joint (usually loosely referred to as the shoulder joint) during wheelchair propulsion. Also, the way in which forces are applied to the hand rims appears to play an important role. Experiments in which the propulsion forces were measured have shown that the direction of the applied forces did not agree with the most optimal direction in terms of power production, i.e. the direction tangential to the hand rims. Fig. 2 illustrates the actual vs the mechanically optimal force direction. Surprisingly, this apparently in mechanical terms suboptimal direction of actual force application was found for athletes as well as untrained subjects [39,54,69,71,99, 100]. It appears that this particular manner of force application is the most efcient force application technique. In other words, subjects appear to adopt the technique that demands the least energy, given the mechanical constraints of the wheelchairuser combination [101]. 4.1. Anatomy The human arm is, contrary to the human leg, not specialized. In contrast, the arm can be used for a large diversity of tasks, varying from manipulation of small objects to handling of heavy materials. In addition, the human arm has a large range of motion. From an ana-
Fig. 2. Illustration of the direction of the propulsion force during normal wheelchair propulsion and the relation with the most effective force direction.
tomical view, the difference in function between arms and legs is well visible in the difference in structure between the shoulder girdle and the pelvis. As stated before, the arm has a large range of motion, as allowed by the loose connection of the scapula to the trunk. Because the scapula is able to slide and rotate over the surface of the rib cage, it is possible to move the base of the arm, the GH joint. This leads to a dramatic increase in the range of motion of the arm. Of course, the inter-muscular co-ordination of the muscles that connect the scapula and humerus to the trunk is extremely important in this. A second reason for the large range of motion of the arm is the fact that the GH joint is shaped as a small and shallow cup (the glenoid) and a large saucer (the humeral head). The cup and saucer are connected by strong, but loose ligamentous tissue. The joint structure allows for rotation in three directions, as well as some translation. As a result, the range of motion of the arm is already quite considerable if the scapula is xed. Despite the fact that the GH joint is loose, spontaneous (sub)luxation seldom occurs. It is assumed that this is the result of muscular control by the rotator cuff muscles. It is evident that good co-ordination between these muscles will be of high importance. Also, athletes who have an incomplete shoulder muscle system, and for whom muscular control is hampered, will be at risk regarding shoulder (sub)luxations [102]. Campbell and Koris diagnosed 24 patients with a cervical spinal cord injury with acute and chronic shoulder pain. Of the 13 patients (15 shoulders) with chronic shoulder pain, eight had (multidirectional) instability problems; contracture or capsulitis was seen in three.
720
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
Shoulder and wrist complaints are very common within the wheelchairuser combination. Recent publications state that at least 50% of the wheelchair users suffer from wrist complaints. About 3050% of this group has problems with their shoulders [94]. A later study indicated even higher prevalence rates of up to 72% for complaints in one or both areas [95]. The high prevalence of complaints is a clear indication that the mechanical load of wheelchair propulsion must be unfavorably high. One of the reasons for the high mechanical load can most likely be found in the fact that much muscular effort is needed for stabilization of the shoulder mechanism and especially for prevention of shoulder luxations. These extra muscular forces would then lead to overload of one or more of those muscles, but also to high compression forces in the GH joint, which in turn might lead to damage to joint cartilage. To get an impression of the mechanical load and the underlying mechanisms, a biomechanical model is a prerequisite. For calculation of the extra forces that would be necessary to stabilize the shoulder, a model would be required that not only is able to calculate net joint torque, but also to calculate individual muscle forces. 4.2. Biomechanics Biomechanics is a powerful tool in the mechanical analyses of the human musculoskeletal system. In biomechanics, one often uses the inverse-dynamic modeling approach. The inverse-dynamic modeling approach takes its starting point, contrary to the direct-dynamic approach, in the resulting movements and (external) forces. Starting from there, the approach then tries to estimate the forces and torques that have been applied by internal structures and that led to the given movement and forces. Also, the approach can be used to estimate the contribution of individual muscles to driving forces and torques. The input of an inverse-dynamic model comprises anthropometry and the (externally) visible movements and forces. This implies, of course, that these have to be measured. Movements can be measured with simple equipment such as video cameras, but also with sophisticated high-speed automatic systems. Important factors in the quality of input data are the frame frequency and image accuracy. If movements are studied that are predominantly planar, such as long jumping, a two-dimensional analysis and recording of the movement usually sufces. The underlying assumption in that case is that movements in other planes are small and also of lesser importance. For wheelchair propulsion this obviously is not the case. The movements do not occur in one plane and recordings from more than one view are necessary. With the help of special computer algorithms,2 two or more combinations of views
2
can be used to reconstruct a 3D description of the movement. The other necessary sources of input are the externally applied forces. In wheelchair propulsion studies, the forces can only be measured with highly specialized equipment. For wheelchair propulsion, only a few research centers in the world have that equipment. Both in the USA and in Taiwan, research groups use an instrumented wheel for their research [1719,21,5154,69 72,75]. The group of Woude and Veeger at the Vrije Universiteit in Amsterdam uses a wheelchair simulator [68,76,103]. Most inverse-dynamic models are capable of calculating the net joint torque and power [17 19,52,64,70,71,75]. Net torque values give a good indication of the net muscular forces that are needed around a joint. However, these torques are net values, which implies that they are the sum of all muscle forces around that joint. Net torque values are thus likely to be underestimations of the actual muscle forces. If, for instance, two antagonists produce the same force against the same torque arm, the resulting net torque will be zero, while the sum of muscle forces is not. In the shoulder, it is likely that, because of the need for sufcient joint stability, antagonists will be active at the same time. In analyses of muscle function in the shoulder, a biomechanical model will therefore be needed that estimates the contribution of muscles to net torques and resulting movements. A biomechanical model has been developed which includes muscles of the arm and shoulder. This model can now also be applied to manual wheelchair propulsion [104,105]. 4.3. Propulsion forces Wheelchair propulsion comprises a pushing phase and a recovery phase. During the pushing phase, the hands make contact with the rims and force is applied by the athlete to the rims. Since the hands hold the rims and therefore automatically follow the circular movement of those rims, the movement of the hands and arms can be characterized as a guided movement. In guided movements the forces that are applied by the hands do not directly inuence the trajectory of the hands. As a consequence, it is possible to apply force that is not tangential to the hand rims. Any force that has a tangential force component will contribute to propulsion. The propulsive force can be, but does not have to be, applied tangential to the hand rims. Experimental results have shown that propulsion forces are indeed not tangentially directed. Veeger et al.
formation (DLT). In the DLT procedure, a reference frame with known markers is used to dene the relationship between cameras and 3D positions. Subsequently, the 3D positions of unknown markers can be estimated when at least two camera views are available.
These algorithms are generally based on the direct linear trans-
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
721
[39] introduced the term fraction effective force (FEF) as a measure for the effectiveness of force application. The FEF is dened as: FEF Fm |Ftot|1 100 (%) (5)
where Fm is the tangential force component and |Ftot| is the magnitude of the propulsion force. Table 4 gives an overview of FEF values that were determined in several experiments of the authors. In general, the FEF was below 80%. The data in Table 4 seem to agree with results from Wu et al. [54], who reported values of 47 49% for riding at a self-selected pace on level ground and average FEF values of 6374% for riding on a ramp of 2.97.1. They also appear to agree with results of Boninger et al. [70], who found values of 5254% for the force ratio F2 /F2 , which is a slightly different dem tot nition for the FEF than is used here. Both Boninger et al. [70] and Wu et al. [54] use the term mechanical efciency when describing the force direction. Also, they view the force as being misdirected. Since mechanical efciency has historically been used in physiology to describe the ratio between external energy production and consumed metabolic energy, the term efciency should not be used. But, more importantly,
the suggestion that the force direction is inefcient and misdirected might well be based on a misconception of the interaction between athlete and wheelchair. In our view [99,105,106], apart from the fact that a more vertically directed force will contribute more to the required friction between hand and rim, the force direction is in fact the most optimal force direction, given the mechanical constraints of the human musculoskeletal system and the interaction with the wheelchair propulsion system [78,107]. In other words, the chosen force direction is the result of the most efcient propulsion technique possible. To illustrate this concept, Fig. 3 depicts two possible conditions. One is the condition in which the mechanically most effective force is applied (a) and the other is the usually measured condition (b). If a wheelchair user were to propel the wheelchair with a force that was directed following Fig. 3(b), the force would have to be generated through an anteexion torque around the shoulder, in combination with an elbow exion torque. These torques are shown as solid lines. On the other hand, the elbow has to be extended (dashed lines) to follow the hand rims in order to be able to apply force on those rims. As a consequence, the
Table 4 Torque, power and FEF for isometric, submaximal and sprint tests on a stationary wheelchair ergometera Test Subject N Speed (m s 1) Submaximal Veeger et al. [82] Power output (W) (std) FEF (%) (std)
AB
AB
Dallmeijer et al. [112]
NWA (C5C7) NWA (T6L4) WA (male) WA (female) AB NWA NWA (C4C8) (T1T5) (T6T10) (T11L4)
12 12
0.56 0.83 1.11 1.39 0.83 1.11 1.39 1.67 0.83 1.11 1.39 1.67 0.83 0.83 1.11 1.11 2.20 2.0 1.97 2.2 1.45 1.95 2.35 2.15
26.6 36.4 46.7 58.9 18.2 19.1 18.7 19.2 37.1 38.1 38.1 38.3 7.8 13.7 27.1 46 108 66 96.0 100 43.8 94.4 122 98.3
(4.9) (5.7) (7.1) (7.7) (3.2) (4.3) (3.1) (4.6) (4.1) (6.4) (6.8) (7.1)
81 78 73 75 72 68 67 61 70 72 72 67 53 57 71 77 52 53 57 61 50 59 59 59
(7) (7) (9) (10) (9) (13) (10) (10) (11) (9) (13) (8)
77
30 s sprint Woude et al. [135] Veeger et al. [100] Dallmeijer et al. [136]
50 17 10 9 6 5 5 7
(45) (32) (8.8) (29.4) (24.6) (30.2) (20.4) (22.5)
(9) (10) (4) (16) (12) (6) (7) (12)
AB: able bodied; NWA: non-wheelchair athletes; WA: wheelchair athletes.
722
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
In order to further reduce mechanical loading during wheelchair propulsion, design aspects of the wheelchair user interface should be considered such that these changes lead to a more effectively applied force (with prevention of the conict between movement direction and torque production around the elbow). 4.4. Torque applied by the hands onto the hand rims Next to a propulsion force, the hands can also apply a torque on the hand rims. This torque can be imagined as a combination of a pushing force at the level of the wrist and a pulling force at the level of the index nger. The magnitude of component of the torque by the hands onto the hand rim surface can be derived from the differences between forces applied on the hand rims and the torque around the wheel axis (Fig. 4). When only a force is applied by the hands (Ftot in Fig. 4), the tangential component of the force that is applied on the rims (Feff) should equal the torque divided by the wheel radius (Fm). The difference between both equals the hand moment (Mh). There is some uncertainty in these estimations, however, since the exact value will be dependent on the point of force application in the hands [17,53,77]. From our estimations it became clear that the magnitude of this torque could become as high as 40% of the total propulsion torque. Unfortunately, the direction of the torque is generally directed against the propulsion torque for most of the push phase. Subjects appeared to work against themselves [77]. One of the possible reasons for this activity might be the need to keep suf-
Fig. 3. Illustration of the mechanically most effective force direction (a) and the actually applied force direction (b). The solid lines indicate the net moments around the shoulder and elbow, the dashed lines indicate the rotation direction in those joints.
elbow exors have to apply force against stretch, which is highly inefcient. It is clear that the contribution of elbow exors will increase the effectiveness of the propulsion force, but that the total force will be smaller. A second aspect of this force direction is that the strong elbow extensors cannot be used. The conditions in Fig. 3(b) depict the force direction with which no conict between torque direction and movement direction occurs. This is the direction that is generally found. The assumption seems justied that this apparently inefcient form of propulsion is based on the most efcient solution, given the mechanical constraints of the system. The production of negative power is prevented and the strong elbow extensors can be used. The above assumption will have consequences for the choice of methods to raise the low level of efciency of wheelchair propulsion. Training of wheelchair propulsion technique may not simply be focused on the improvement of effectiveness of force application. In cycling it has been shown that instruction to direct forces more effectively did not lead to higher efciency levels [108]. A recent experiment on feedback based learning of a mechanically supposedly better more tangential force direction in a group of non-wheelchair users on the wheelchair ergometer has shown that subjects are able to improve the effectiveness of force application towards a more tangential direction, but initial physiological results indeed indicate that there is no positive effect on the gross mechanical efciency of task performance [78], as was also expected on theoretical notions presented above and by Rozendaal [107]. It does however not imply that exercise and training which both also involve a learning process cannot improve task prociency, as well as task efciency. The results of Rodgers et al. [64] and Dallmeijer et al. [109] do suggest a training or learning effect as a consequence of repeated (long-term) wheelchair use. Dallmeijer et al. showed initial results of training on simple technique parameters such as timing and stroke angle in non-wheelchair users. No changes in force production parameters were found however.
Fig. 4. Illustration of the principle of the hand moment. Mh: hand moment; Feff: effective component of the propulsion force (Ftot); Fm: effective force determined from the propulsion torque (M). MCII is the (arbitrary) point of application.
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
723
cient contact with the rims for force application. As a consequence, the hands are being forced from radial deviation to ulnar deviation while the wrist exors are likely to be active [77]. The application of a counter productive hand torque is not only likely to be inefcient, but also likely to be an important factor in the occurrence of carpal tunnel syndrome (CTS). Important predisposing factors for CTS are direct pressure on the carpal tunnel, extreme wrist positions and nger exion activity (or tension on the tendons running through the carpal tunnel). Recent experiments [74] have shown that during wheelchair propulsion large wrist angles occur, even in combination with nger exor activity. Especially peak ulnar and radial deviation were close to their range of motion values. Table 5 gives the average peak values, in combination with indicative values for the active range of motion in the wrist joint. The authors concluded that at least three factors that could lead to CTS occur during wheelchair propulsion: extreme wrist excursions, occurring also in combination with nger exor activity, and within a highly repetitive movement. In combination with the likeliness of a considerable direct pressure of the rim on the carpal tunnel, three predisposing factors for CTS can be discerned. The suggestion, however, that a glove might reduce the risk for CTS [74], could not be proven [92]. Regarding the inuence of the hand torque on efciency, it should be mentioned here that experiments in which a slightly wider rim tube was used, efciency signicantly improved. However, no signicant reductions in the magnitude of the hand torque were found [77]. 4.5. Modeling results Modeling results from several authors have indicated that the largest joint torques are produced around the shoulder complex. Veeger et al. [39] reported peak shoulder exion torques of 35 N m, in combination with peak adduction torques of 20 N m. Peak elbow extension
Table 5 Peak wrist angles (degrees), averaged over nine subjects and six experimental conditions, were either calculated over the full push angle, or over that part of the push angle where nger exor activity was recorded. The numbers in parentheses represent the standard deviation [74] Angle Peak angle Peak angle+exor activity 16 32 22 13 (15) (16) (11) (10) Active range of motion (average from literature) 76 66 35 21
Flexion Extension Ulnar deviation Radial deviation
14 34 24 13
(18) (16) (11) (12)
torques were 10 N m. Wu et al. [54] also reported largest torques around the shoulder joint, but predominantly as a shoulder exion torque. The peak shoulder and elbow torques were surprisingly small (43 and 6.1 N m, respectively, for riding up a 2.9 ramp). Rodgers et al. [52] found a large shoulder exion torque of approximately 30 N m and elbow extension torque of approximately 10 N m. When these values are interpreted, it should be kept in mind that the shoulder data are in fact values that are based on a simplication of the shoulder complex as one ball-and-socket joint. It is likely that inclusion of the scapula as a separate segment will have a lowering effect on the torques estimated in this way. However, the large torques around the shoulder complex indicate large muscle forces. This is supported by electromyographic data by Mulroy et al. [110], who found the highest EMG activity in the supraspinatus muscle and sternal part of pectoralis major. Wrist joint torques were reported by Boninger et al. [71]. They calculated the largest peak torques around the wrist in the direction of ulnar deviation (16.6 N m at 1.3 m s 1 traveling velocity in a standard wheelchair). The peak wrist extension torque was smaller, but still 10.4 N m (1.3 m s 1). These relationships between ulnar deviation and extension are supported in other publications [52]. The large wrist torques and especially the large ulnar deviation torque can be seen as another risk factor for the occurrence of CTS. The previously mentioned musculoskeletal model of the upper extremity has been applied to a quasi-static approximation of wheelchair propulsion [106]. The wheelchair push was simulated in different quasi-static stages: asking the subjects to push the hand rim in different positions ( 15 (starting position), 0 (top-deadcenter), 15, 30, 45 and 60). Also, measurements were performed against resistances from 0 to 40% of the maximal push force on the rims (24420N, N=10). The model was then used to estimate the compression force in the GH joint and to compare those values with the net forces that work on the joint. Net forces are dened as the result of all external forces that are generally the combination of the propulsion force and gravity. Compression forces are the net forces and the forces that work on the joint internally, by muscles and ligaments that work together to produce the propulsion force. The results of these calculations are given in Fig. 5. From the calculations it followed that the compression force in the GH joint could reach high values, close to 2000 N or 200 kg, even during these submaximal exertions. One of the main reasons for this high compression force was the additional muscle force that was needed to stabilize the GH joint (Fig. 6). Forces in the rotator cuff muscles were high, while at the same time their contribution to the external torque around the GH joint was small. This implied that they were primarily active to
724
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
Fig. 5. Average results for the net forces on the GH joint (left) and the compression forces in the joint (right) (adapted from Helm and Veeger [106]).
Fig. 6. Estimated muscle forces of a selection of shoulder muscles, plotted together with the compression force in the GH joint. Supr: supraspinatus; Infr: infraspinatus; TeMi: teres minor; Subs: subscapularis; DeAn: deltoideus pars anterior; PeTh: pectoralis major, pars thoracale; PeCl: pectoralis major, pars claviculare (adapted from Veeger and Woude [73]).
compensate destabilizing effects of the prime movers, the deltoid and pectoral muscles. The dynamic capabilities of the armshoulder model, and its contribution to a possibly better understanding of the mechanical strain to the neuromuscular system in hand rim wheelchair propulsion under different boundary conditions, is shown by Veeger [111] and Helm and Veeger [105]. 4.6. Effect of an incomplete muscle system Up till now, the descriptions that have been given of biomechanical factors that inuence wheelchair propulsion, have been of a general character and based on a user group with full control over their upper extremities and trunk. It is expected that for those wheelchair users who have an incomplete musculoskeletal system, the problems will exacerbate. Adequate stabilization of the GH joint will, for instance, become more difcult and the risk of dislocation of the joint will be high. There has been, up till now, no direct proof for this assumption, but a study by Campbell and Koris [102] may serve as
an illustration. In this study a group of 24 patients with cervical spinal cord injury were studied, eight of which were diagnosed with a chronically unstable shoulder. Recently, Dallmeijer et al. [112] found that effectiveness of force application (FEF) in submaximal wheelchair propulsion of persons with tetraplegia is even lower than in persons with unimpaired arm function. FEF values of around 50% were found. The total force vector showed a larger, latero-medial directed and ineffective force component. 4.7. Concluding remarks Biomechanics is a strong tool in helping to understand aspects of performance, technique and mechanisms of overuse injury in groups of individuals, even with differing functional abilities. One needs to be careful, however, with the results of a study at this stage. Measurement does not equal understanding. Even more than in physiologically oriented studies, biomechanical studies concentrate on small numbers of subjects. Also, one needs to realize that a mechanical frame of reference
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
725
does not necessarily comply to biological phenomena that are observed. Above all, one needs to realize that biomechanical modeling has its limitations: models remain models. At this stage model ndings cannot be individualized. There is no evidence based consensus regarding what is an optimum biomechanical task performance. A combined research approach from within biomechanics and physiology (and engineering) seems most productive. To more clearly dene injury mechanisms onto the musculoskeletal system, obviously requires longitudinal study as well.
briey discuss the sources of energy losses: rolling resistance, air resistance an internal friction. 5.1. Rolling resistance In daily use conditions, rolling resistance generally is the major resisting force. Below relative head wind conditions of 2 m s 1, air drag is still negligible. Rolling resistance can be determined in different manners. A coast-down technique as described by McLaurin [113] is frequently used to determine rolling friction characteristics of the wheelchair in combination with different oor surfaces, or the effect of combined air and rolling resistance. A second method is the drag test. Also, rolling resistance can be measured by measuring of the push force as is exerted by a wheelchair attendant to evaluate different oor surfaces (Fig. 7). Apart from oor surface, rolling friction is essentially dependent on the characteristics of the wheels and tires; rolling resistance is lower for wheels with a larger radius and for harder tires. Rolling resistance can be expressed by the following equation: Froll m1(N1R1) m2(N2R1) (N) 1 2 (7)
5. Vehicle mechanics Vehicle mechanics is an essential element in active wheelchair performance. When mechanical properties of the wheelchair are discussed, however, one should always consider the effect of those properties in conjunction with the user. The mechanical performance of a wheelchair is subject to rolling friction, air drag and internal friction of the wheelchair. Task load can be expressed as external power, or the energy per unit time that is required to maintain the speed of the wheelchairuser combination. With the help of a so-called power balance, the forces and energy sources responsible can be systematically evaluated [30,31]. The power balance for wheelchair propulsion can be expressed as: Po (Froll Fair Fint mgsin a ma)v (W) (6)
where Po is the external power output, a is the acceleration of the system, m is the mass of the wheelchair and user, and a is the angle of slope or inclination. If a wheelchair is kept at a constant speed, the athlete has to produce a certain amount of energy per unit time, or power. This is called external power (Po). This external power is produced by the user and requires a much higher amount of internal power. The external power output is necessary to overcome energy losses in the system. The wheelchairuser combination will lose energy in the form of rolling resistance, air resistance and internal resistance in the mechanical structures of the chair. When more external power is produced than is needed to overcome these losses, the chair will accelerate. The magnitude of acceleration will be dependent on the weight of the chair (ma). Also, the surplus of external power can be used to overcome a slope (mg sin a). On the other hand, negotiating a slope will, at a given external power output, lead to slowing down of the system. The terms ma and mg sin a should not be considered as straight losses since they will work both ways. Energy, invested in acceleration or climbing, will be harvested when coasting or descending. In the following, we will
where R1 and R2 are the radii of the front and rear wheels; N1 and N2 indicate the relative weight on those wheels; and m1, m2 are the friction coefcients. The magnitude of the friction coefcients is related to the amount of deformation of tire and oor surface. This deformation dissipates energy [6,7]. Deformation is dependent on tire pressure, tread and prole, or wheel diameter, but also on wheel alignment (Table 6). Wheel toe-in or toe-out has a considerable effect on rolling resistance [114]. For camber this is not so clear. It appears that, according to the experimental results of Veeger et al. [38] and OReagan et al. [114] camber of the rear wheels has no negative effect on rolling friction. However, Weege [115] advocates the opposite on the basis of theoretical considerations. A special, frequently encountered problem in daily wheelchair use and racing is the effect of a side slope [115,116]. The wheelchair generally will have the tendency to coast down a slope, which makes the steering of the wheelchair complicated and increases rolling resistance due to the effect on the alignment of the front casters. For that purpose track and racing wheelchairs are equipped with steering mechanisms that x the direction of the front wheel in a pre-set direction. 5.2. Air resistance The second important factor in the power balance equation (Eq. (6)) is air resistance. In wheelchair racing this factor is by far the most important source of energy losses. Air resistance is dependent on the drag coefcient
726
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
Fig. 7. Rolling resistance measured with an attendant push wheelchair mounted with a 70 kg test dummy on different oor surfaces (adapted from Woude et al. [137]).
Table 6 Different characteristics of the wheelchairuser combination and their inuence on rolling friction Characteristics Body mass Wheelchair mass Tyre pressure Wheel size Hardness oor Camber angle Toe-in/out Castor shimmy Center of mass over large rear wheels Folding frame (vs box frame) Maintenance Effect on rolling friction ?
Next to frontal area reduction, adaptation of the seat position and orientation of the segments of the body, and the application of skin suits will inuence the drag coefcient. 5.3. Internal friction Energy losses within the wheelchair are caused by bearing friction around the wheel axles and in the wheel suspension of the castor wheels and possibly by the deformation of the frame in folding wheelchairs during the force exertion in the push phase. Bearing friction generally is very small, and given that the hubs have annular bearings and are well maintained and lubricated, this friction coefcient will not exceed 0.001 [10]. However, the losses in ill-maintained bearings can be considerable. An experimental comparison of one subject with a worn out castor wheel bearing in his racing wheelchair with seven companion racers in a similar design wheelchair showed that the mean values for power output of the seven subjects (with a higher overall mean body weight) was 20 W lower at a velocity of 3.3 m s 1, which implies at a theoretical gross mechanical efciency of 8% an increase in oxygen consumption of 0.75 l min 1 for the subject in the wheelchair with the worn-out castor. This occurred, despite the fact that this subject had a lower body weight than the other seven subjects. An unknown aspect of internal energy dissipation is the loss of propulsion energy due to deformation of the frame elements. This will clearly be possible in folding wheelchairs, but has not been addressed empirically. The use of levers and cranks does introduce a chain, chain wheel and gearbox related friction. Whitt and Wilson [121] indicate a possible loss of energy of 1.5% in chain transmission.
(Cd), frontal plane area (A), air density (d) and velocity of the air ow relative to the object (v): Fair
1 2
dACdv2 (N)
(8)
As mentioned earlier, air resistance will be of minor importance at low speeds, but at high speeds and/or wind velocities air resistance will be the most important source of resistance. Following Abel and Frank [117], at slow speed (1 m s 1) air drag will be below 1 N, while at 5 m s 1 the drag force due to air resistance is 14 N, which implies an average power output of (514=) 70 W for wind resistance only at that wheelchair speed. It is obvious that the frontal plane area is dependent on the posture of the athlete. Although a wind tunnel experiment has been performed [118] as well as empirical measurements [119,120], no recent gures on air resistance have been published in association with contemporary wheelchair sitting posture and propulsion technique. However, from cycling or speed skating many new developments were transferred to wheelchair racing.
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
727
5.4. Slope and acceleration Both slope and acceleration effects are no straight loss components in the power balance equation. Energy invested in overcoming a hill, or increasing velocity will be returned in descents and when coasting. It should, however, be kept in mind that the invested potential energy will be returned against a larger head wind and thus at much larger power losses due to air resistance (Eq. (8)). As a result, maintaining the same average velocity will require more energy than when compared with wheeling on a level surface. Although body weight and wheelchair weight have a small effect on rolling resistance, they have a considerable effect on the slope component and the acceleration component. Acceleration potential is inversely related to total weight at a given power output (acceleration will be slower when the weight of the system is larger). Also, weight is linearly related to power output in climbing. Of course, this extra investment will be returned partially during descents, but will still lead to higher losses. Wheelchair weight can be inuenced through proper technology and lightweight materials. Their relative contributions must be weighed in the light of frequently seen individual overweight, however. Given the fact that performance will benet from an as low as possible drag force, a racing wheelchair should meet the following criteria: xed customized frame; xed foot/leg support; custom made and tapered front end; custom frame angle of 80 or more; camber house; xed backrest; xed clothes protectors; weight: as low as possible; rear axis: customized seat angle and height, and rear wheel camber angle: 612. Weight distribution should be such that dynamic balance is maintained, even at high acceleration and when negotiating slopes. In other words, the center of gravity should not be too close to the rear axis. 5.5. Concluding remarks Apart from the innate biological tools of the active wheelchair user, performance will be strongly inuenced by the mere mechanics of the wheelchair. In wheelchair sports, fair competition is not only dependent on proper classication of the athletes alone, but also on a quality regulation of the wheelchair, especially for those athletes with limited nancial and scientic resources.
mechanical efciency. Also, the experiments focusing on the interfacing have proven the possible role of optimization and the effects of interfacing on propulsion technique. Examples of these are: rim size, gear ratio [40,122], rim tube diameter [65,67] and seat height and position [20,44,63,123]. Of course, the propulsion mechanism (levers, rims or cranks) has a denite inuence on performance [31,45,63,124,125]. 6.1. Rim radius or gear ratio The hand rim radius is in fact a gearing level. Smaller hand rims will result in a larger force and smaller hand velocity at a given traveling speed. It is logical that different task conditions will require different hand rim diameters or gearing levels: groups of well-trained subjects may want a gearing which enables them to compete at high velocities, whereas a steep incline for physically less able subjects will demand a low gear. The relevance of different gear ratios in hand rim wheelchairs is stressed by the results of different experimental studies [40,65,67]. Veeger et al. [40] showed that at equal submaximal power output, a higher mechanical advantage (0.43 0.87), i.e. a higher hand velocity and simultaneously a lower mean resisting force led to a higher cardiorespiratory response. Simultaneously, the increase in linear hand velocity during the push phase led to a decrease in effective force, which decreased from 71 to 58%. In addition, the amount of negative work at the beginning and end of the push increased with a higher mechanical advantage. Application of a variable gearing in hand rim wheelchairs is worth considering, but complicated, technically speaking. However, different rim diameters are more common, especially in track wheelchairs. In wheelchair sports, athletes tend to individualize their choice of hand rim size, tube diameter and prole. To study the physiological effects of rim size, Woude et al. [37] conducted an experiment with a racing wheelchair and ve different rim diameters in which track athletes participated at speeds up to 4.2 m s 1. Rim diameter varied from 0.30 to 0.56 m. Results showed that the largest rim led to the highest physiological strain and lowest efciency levels. Heart rate showed a mean difference of 20% (1020 b min 1) between the smallest and the largest rim size. Again the linear speed of the hand rim limited performance: ve out of eight athletes were unable to perform at a velocity of 4.2 m s 1, using the largest hand rim (power output did not exceed 50 W!). The full advantage of variable gearing is met in handbikes and different lever systems. However, the appropriate choice of ratio will be power and velocity dependent. More systematic studies should be conducted with respect to the effects of rim size, tube diameter, form and prole in a physiological and biomechanical context
6. Wheelchairuser interface The interface between wheelchair and user will inuence performance. The interaction of the musculoskeletal system with the form and geometry of the propulsion mechanism and the seat conguration has been shown to inuence the energy cost, physical strain and the gross
728
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
for different groups of wheelchair users. The need for a choice in exchangeable rims is however clear. 6.2. Camber The majority of sports wheelchairs are equipped with cambered rear wheels. Wheelchairs with cambered wheels are generally said to perform better in track events [126]. There appears to be a biomechanical rationale for the suggested better performance with cambered wheels: with the top of the wheels as near as possible to the trunk the rims are in a plane more or less passing through the shoulder joint. This would prevent the upper arms from abducting in the frontal plane, thus reducing the static effort of the shoulder muscles. The effective force vector can also be directed as closely as possible to the shoulder joint. Whether these assumptions are valid, was studied by Veeger et al. [38] for basketball wheelchair use during propulsion at speeds of 0.561.39 m s 1 on a motor driven treadmill (N=8 nonwheelchair users). During four subsequent exercise tests the camber angle varied randomly from 0 to 3, 6 and 9. The cardio-respiratory parameters indicated no positive or negative effect of camber angle in this wheelchair model. Similar ndings were seen for the kinematics: no change in abduction angle was evident with camber angle. The electromyography signal even showed an absence of activity of the major shoulder abductor (m. deltoideus pars medialis) during the push phase. The authors explained this phenomenon by stating that the abduction, that occurs during the push phase, is not an active process, but a side effect of the action of the major shoulder muscles (mm. pectoralis major and the deltoideus pars anterior). Their activity would lead both to anteexion as well as abduction and endorotation, because of the closed kinetic chain that exists between the hand and the shoulder in the push phase. It thus appears that camber does not affect the functional load. However, the positive effect of camber on stability is relevant, as well as the fact that the hands are protected when passing along objects. 6.3. Other propelling mechanisms A relatively unknown propulsion mechanism is the hubcrank, a device that allows a continuous motion of the hand around the wheel hub of the rear wheels of a track or racing wheelchair. Thus, hubcranks allow continuous force exertion onto the wheel hubs. The hubcrank has a well-tted handgrip that rotates freely around an axle perpendicular to the crank and adapts itself to the orientation of the hand. The crank has a free wheel. It is typically used in training of athletes, in opencompetition sports events and in recreation. The efcacy of this device was studied in a group of non-wheelchair users. It turned out that the cranks led to a signicantly
Fig. 8. VO2 (handrim minus huberank) as a function of power output for studies of Vlies et al. [138] ( ) and by Woude et al. [45] ( ).
lower strain compared with similarly sized hand rims (Fig. 8). Gross mechanical efciency was up to 3% higher than for hand rims. Comparable trends were seen in a pilot study for a small group of trained wheelchair athletes [45]. The positive effects using the hubcrank may be explained by the following notions: The continuous circular motion allows both push and pull actions, thus reducing the periods during which no power is generated (as in hand rim propulsion during the recovery phase). The continuous circular motion allows for contributions of both exor and extensor groups, and thus spreads out the load over more muscle groups. The hand and wrist have a more natural orientation to the lower arm (the handgrip adapts to the spatial hand orientation). As a consequence, the coupling of the hand to the propulsion mechanism is easier, with no counteracting hand moment. In addition, the grip force of the nger exors might be lower. This may lead to a reduction in strain in the carpal tunnel.
Fig. 9. Gross mechanical efciency in different propulsion mechanims (adapted from Woude et al. [31]).
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
729
Table 7 Summary of typical functional wheelchair characteristics for the handrim, crank, lever and hubcrank propelled wheelchairs, based on the reviewed literature [42]a Hand rim Basketball Max ME (%) Strain CVS b Strain MSS b Risk RSIb Top speed (km h 1) Mass (kg) Coupling of the hand Effectiveness of force direction Bi-modal force cycle Continuous force transfer Manoeuvrability Steering Braking
a b
Crank Racing 8 High High High 30 8 + + + + 13 Low Low Low? 30 15 ++ +? + + +
Lever
Hub
10 High High High 15 10
++ ++
13 Low Low Low? 30 15 ++ ++? + + +
12 Low? Low? Low? 30 8 + +? + +
: not good, not bad/average; +: (very) positive/good; : (very) negative/bad; ?: is not supported with research ndings. CVS: cardiovascular system; MSS: musculoskeletal system; RSI: repetitive strain injuries.
In conclusion, the hubcrank has some clear advantages over the hand rim. Its use to date is however restricted to track wheelchairs, outdoor use, and to procient wheelchair users. The wheelchair is hard to steer, braking is more complicated and its increased width (+0.15 m) complicates indoor use. These aspects may be improved with simple design alterations. Overall the above-mentioned mechanisms of an increased strain and reduced efciency in hand rim propulsion do hold for different alternative modes of propulsion, such as lever propulsion or the more ordinary handbike. In ofcial wheelchair track events (World Games, Paralympics) other propulsion mechanisms than hand rims are not allowed. This is rather unfortunate, since hand rim propelled wheelchairs are inefcient compared with alternative modes of wheeled ambulation, such as levers or cranks [42]. In Fig. 9, a comparison between a three-wheeled synchronous lever, a conventional crank propelled wheelchair and two hand rim propelled wheelchairs (a daily-active and sports wheelchair) has been made with respect to oxygen uptake (N=10 non-disabled subjects, v=0.96 m s1, slope of 03). Both cranks and levers are considerably less straining. A brief overview of their different characteristics is given in Table 7. Despite the higher power output of the quite heavy tricycles, heart rate and oxygen cost were signicantly lower. The crank and lever propulsion mechanisms appear appropriate for outside use at relatively high velocities, as well as for longer distances, both for well trained as well as sedentary individuals [27]. Even those with serious functional limitations to the upper extremity and trunk will benet [28]. Athletes with C6C8 lesions reached mean power output of 5525 W, whereas those with lower lesions attained
values of 12926 W during a maximal exercise test using their tricycle on a motor driven treadmill. Optimization of gear ratio, lever length, handgrip and spatial orientation of the crank or lever should, however, receive systematic attention [29,31,65,123,125]. Preferably, research should take a combined biomechanical and physiological perspective in order to further ne-tune the propulsion mechanism to the individual characteristics and conditions of use. The current revival of contemporary lever and crank propelled wheelchairs for (open category) sports events and for recreational purposes is stimulating and will require new sports regulations in competition. 6.4. Conclusion Systematic combined physiological and biomechanical study of the wheelchairuser interface helps us to understand and identify performance determining as well as limiting characteristics, thus increasing performance in active wheelchair use. Presented and other interface characteristics (seat height/orientation) require further detailed analysis in relation to functionality. Thus, long-term ailments of the musculo-skeletal system related to a wheelchair dependent lifestyle may be discerned and eventually prevented. References
[1] Woude LHV et al. Manual wheelchair propulsion. In: Zatsiorski V, editor. Biomechanics of sport: performance enhancement and injury prevention. Oxford: Blackwell Science, 2000. [2] Cooper RA. Wheelchair racing sports science: a review. J Rehab Res Dev 1990;27:295312.
730
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
[3] Peizer ED, Wright D, Freiberger H. Bioengineering methods of wheelchair evaluation. Bull Prosth Res 1964;10:70100. [4] Brubaker CE, McLaurin CA. Wheelchair mobility 19761981. REC, University of Virginia; 1981. [5] Staros A. Testing of manually-propelled wheelchairs: the need for international standards. Prosthetics Orthotics Int 1981;5:7584. [6] Kauzlarich JJ, Thacker JG. Wheelchair tire rolling resistance and fatigue. J Rehab Res Dev 1985;22(3):2541. [7] Kauzlarich JJ. Wheelchair rolling resistance and tyre design. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:15872. [8] Boosfeld C. Messung der Belastung von Rollstuehlen im Labor und Feld mit einem ortsunabhaengigen Mikrocomputer-system Biomedizinische Technik. Forschungsberichte fuer die Praxis Band I Schiele and Schoen; 1988. [9] Bougie T, Davies A. Wheelchair: research, evaluation, and information. Commission of European Communities, COMAC BME, Edizione Pr Juventute, Milan; 1988. [10] Frank TG, Abel EW. Drag forces in wheelchairs. In: van der Woude LHV, Meijs PJM, van der Grinten BA, editors. Ergonomics of manual wheelchair propulsion: state of the art. Amsterdam: IOS Press, 1993:25567. [11] Brouha L, Krobath H. Continuous recording of cardiac and respiratory functions in normal and handicapped people. Human Factors 1967;9:56772. [12] Voigt ED, Bahn D. Metabolism and pulse rate in physically handicapped when propelling a wheelchair up an incline. Scand J Rehab Med 1969;2:1438. [13] Brauer RL, Hertig BA. Torque generation on wheelchair handrims. Am Soc Mech Eng AMD 1981;43:1136. [14] Sanderson DJ, Sommer HJ. Kinematic features of wheelchair propulsion. J Biomech 1985;18(6):4239. [15] Cooper RA. An exploratory study of racing wheelchair propulsion dynamics. Adapt Phys Act Quart 1990;7:7485. [16] Cooper RA. A systems approach to the modelling of racing wheelchair propulsion. J Rehab Res Dev 1990;27(2):15162. [17] Cooper RA, Robertson RN, VanSickle DP, Boninger ML, Shimada SD. Projection of the point of force application onto the palmar plane of the hand during wheelchair propulsion. IEEE Trans Rehab Eng 1996;4(3):13342. [18] Cooper RA, Boninger ML, VanSickle DP, Robertson RN, Shimada SD. Uncertainty analysis for wheelchair propulsion dynamics. IEEE Trans Rehab Eng 1997;5(2):1309. [19] Cooper RA, Robertson RN, VanSickle DP, Boninger ML, Shimada SD. Methods for determining three-dimensional wheelchair pushrim forces and moments: a technical note. J Rehab Res Dev 1997;34(2):16270. [20] Hughes CJ, Weimar WH, Sheth PN, Brubaker CE. Biomechanics of wheelchair propulsion as a function of seat position and userto-chair interface. Arch Phys Med Rehab 1992;73:2639. [21] Rodgers MM, Gayle GW, Figoni SF, Kobayashi M, Lieh J, Glaser RM. Biomechanics of wheelchair propulsion during fatigue. Arch Phys Med Rehab 1994;75:8593. [22] Ruggles DI, Cahalan T, An K-A. Biomechanics of wheelchair propulsion by able-bodied subjects. Arch Phys Med Rehab 1994;75:5404. [23] Tupling SJ, Davis GM, Pierrynowski MR, Shephard RJ. Arm strength and impulse generation: initiation of wheelchair movement by the physically disabled. Ergonomics 1986;29:30311. [24] Vanlandewijck YC, Spaepen AJ, Lysens RJ. Wheelchair propulsion: functional ability dependent factors in wheelchair basketball players. Scand J Rehab Med 1994;26:3742. [25] Cooper RA. Rehabilitation engineering: applied to mobility and manipulation, Medical Science Series. Bristol: Institute of Physics Publishing, 1995. [26] van der Woude LHV, Veeger HEJ, Rozendaal RH. Ergonomics
[27]
[28]
[29]
[30] [31]
[32]
[33]
[34]
[35]
[36] [37]
[38]
[39]
[40]
[41] [42]
[43]
[44]
[45]
[46]
of manual wheelchair propulsion: a prerequisite for optimum wheeling conditions. Adapt Phys Act Quart 1989;6:10932. Oertel J, Brundig B, Henze W, Engel P. Spiroergometric eldstudy of wheelchair propulsion with different hand-drive systems. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:18790. Janssen TWJ, Dallmeijer AJ, van der Woude LHV. Physical capacity and race performance in handcycle users. J Rehab Res Dev 2001;38(1):3341. van der Woude LHV, Dallmeijer AJ, Janssen TWJ, Veeger HEJ. Alternative modes of manual wheelchair ambulation: an overview. Am J Phys Med Rehab 2001, in press. van Ingen Schenau GJ. Cycle power: a predictive model. Endeavour 1988;12(1):447. van der Woude LHV, De Groot G, Hollander AP, van Ingen Schenau GJ, Rozendal RH. Wheelchair ergonomics and physiology testing of prototypes. Ergonomics 1986;29(1):156173. van der Woude LHV, Hendrich KM, Veeger HEJ, van Ingen Schenau GJ, Rozendal RH, De Groot G, Hollander AP. Manual wheelchair propulsion: effects of power output on physiology and technique. Med Sci Sports Exerc 1988;20(1):708. Goosey VL, Campbell IG, Fowler HE. Symmetry of elbow kinematics during wheelchair racing. Ergonomics 1998;41:18101620. Chow JW, Millikan TA, Carlton LG, Morse MI, Chae W-S. Biomechanical comparison of two racing propulsion techniques. Med Sci Sports Exerc 2001;33:47684. Bennedik K, Engel P, Hildebrandt G. Der Rollstuhl. Experimentelle Grundlagen zur technischen und ergometrischen Beurteilung handbetriebener Krankfahrzeuge. Rheinstetten: Schindele-Verlag, 1978. ACSM. Resource manual for guidelines for exercise testing and prescription. 2nd ed. Philadelphia: Williams & Wilkins, 1993. van der Woude LHV, Veeger HEJ, Rozendal RH, van Ingen Schenau GJ, Rooth F, van Nierop P. Wheelchair racing: effects of rim diameter and speed on physiology and technique. Med Sci Sports Exerc 1988;20(5):492500. Veeger HEJ, van der Woude LHV, Rozendal RH. The effect of rear wheel camber in manual wheelchair propulsion. J Rehab Res Dev 1989;26(2):3746. Veeger HEJ, van der Woude LHV. Load on the upper extremity in manual wheelchair propulsion. J Electromyogr Kinesiol 1991;1:27080. Veeger HEJ, van der Woude LHV, Rozendal RH. Effect of handrim velocity on mechanical efciency in wheelchair propulsion. Med Sci Sports Exerc 1992;24(1):1007. Sawka MN. Physiology of upper body-exercise. Exerc Sport Sci Rev 1986;14:175211. van der Woude LHV, Veeger HEJ, Bouten C, Gwinn T. Aerobic work capacity in elite wheelchair athletes. Am J Phys Med Rehab 2001, in press. Brown DD, Knowlton RG, Hamill J, Schneider TL, Hetzler RK. Physiological and biomechanical differences between wheelchair-dependent and able-bodied subjects during wheelchair ergometry. Eur J Appl Physiol Occup Physiol 1990;60(3):17982. van der Woude LHV, Veeger HEJ, Rozendal RH, Sargeant TJ. Seat height in handrim wheelchair propulsion. J Rehab Res Dev 1989;26(4):3150. van der Woude LHV, van Kranen E, Ariens G, Rozendal RH, Veeger HEJ. Physical strain and mechanical efciency in hubcrank and handrim wheelchair propulsion. J Med Eng Tech 1995;19(4):12331. Cardus D, McTaggart WG, Ribas-Cardus F, Donovan WH. Energy requirements of gameeld exercises designed for wheelchair bound persons. Arch Phys Med Rehab 1989;70:1247.
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
731
[47] Mattison PG, Hunter J, Spence S. Development of a realistic method to assess wheelchair propulsion by disabled people. Int J Rehab Res 1989;12(2):13745. [48] Vanlandewijck YC, Daly DJ, Theisen DM. Field test evaluation of aerobic, anaerobic and wheelchair basketball skill performances. Int J Sports Med 1999;20:54854. [49] Vinet A, Bernard P-L, Poulain M, Varray A, Le Gallais A, Micallef J-P. Validation of an incremental eld test for the direct assessment of peak oxygen uptake in wheelchair-dependent athletes. Spinal Cord 1996;34:28893. [50] Asato KT, Cooper RA, Robertson RN, Ster JF. SMART wheel: development and testing of a system for measuring manual wheelchair propulsion dynamics. IEEE Trans. Biomed. Eng. 1993;40:1340-1324. [51] Cooper RA, Bonninger ML, VanSickle DP, DiGiovine CP. Instrumentation for measuring wheelchair propulsion biomechanics. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:10415. [52] Rodgers MM, Tummarakota S. Three-dimensional analysis of wheelchair propulsion. J Appl Biomech 1998;14:8092. [53] Sabick MB, Zhao KD, An KN. A comparison of methods to compute the point of force application in handrim wheelchair propulsion: a technical note. J Rehab Res Dev 2001;38(1):5768. [54] Wu HW, Su FC. An instrumented wheel for the kinetic analysis of wheelchair propulsion. J Biomed Eng 1998;120:5335. [55] Gass GC, Camp EM. Physiological characteristics of trained Australian paraplegic and tetraplegic subjects. Med Sci Sports Exerc 1979;11(3):2569. [56] Jarvis S, Rolfe H. The use of an inertial dynamometer to explore the design of childrens wheelchairs. Scand J Rehab Med 1982;14:16776. [57] Glaser RM. Exercise and locomotion for the spinal cord injured. Exerc Sport Sci Rev 1985;13:263303. [58] Forchheimer F, Lundberg A. Wheelchair ergometer development of a prototype with electronic braking. Scand J Rehab Med 1986;18:5963. [59] Keyser RE, Rodgers MM, Gardner ER, Russell PJ. Oxygen uptake during peak graded exercise and single-stage fatigue tests of wheelchair propulsion in manual wheelchair users and ablebodied. Arch Phys Med Rehab 1999;80(10):128892. [60] Samuelsson K, Larsson H, Tropp H. A wheelchair ergometer with a device for isokinetic torque measurement. Scand J Rehab Med 1989;21:2058. [61] Theisen D, Franceaux M, Fayt A. A new procedure to determine external power output during handrim wheelchair propulsion on a roller ergometer. Int J Sports Med 1996;17:56471. [62] Digiovine CP, Cooper RA, Bonninger ML. Dynamic calibration of a wheelchair ergometer. J Rehab Res Dev 2001;38(1):4155. [63] Lesser W. Ergonomische Untersuchung der Gestalltung antriebsrelevanter Einussgroessen beim Rolstuhl mit handbetrieb. Duessedorf: VDI Verlag, Reihe 17: Biotechnik nr 28; 1986. [64] Rodgers MM, Keyser RE, Gardner ER, Russell PJ, Gorman PH. Inuence of trunk exion on biomechanics of wheelchair propulsion. J Rehab Res Dev 2000;37(3):28395. [65] McLaurin CA, Brubaker CE. Biomechanics and the wheelchair. Prosthetics Orthotics Int 1991;15(1):2437. [66] Pare G, Noreau L, Simard C. Prediction of maximal aerobic power from submaximal exercise test performed by paraplegics on a wheelchair ergometer. Paraplegia 1993;31:58492. [67] Traut L, Schmauder M. Ergonomic design of the handmachine interface for wheelchairs. In: van der Woude LHV, Meijs PJM, van der Grinten BA, editors. Ergonomics of manual wheel-chair propulsion: state of the art. Amsterdam: IOS Press, 1993:33548. [68] Niesing R, Eijskoot F, Kranse R, den Ouden AH, Storm J, Veeger HE, van der Woude LHV, Snijders CJ. Computer-controlled
[69]
[70]
[71]
[72]
[73]
[74]
[75]
[76]
[77]
[78]
[79]
[80]
[81]
[82]
[83]
[84]
[85]
[86]
[87]
[88]
wheelchair ergometer. Med Biol Eng Comput 1990;28(4):329 38. Robertson RN, Boninger ML, Cooper RA, Shimada SD. Pushrim forces and joint kinematics during wheelchair propulsion. Arch Phys Med Rehab 1996;77:85664. Boninger ML, Cooper RA, Robertson RN, Shimada SD. Threedimensional pushrim forces during two speeds of wheelchair propulsion. Am J Phys Med Rehab 1997;76(5):4206. Boninger ML, Cooper RA, Robertson RN, Rudy TE. Wrist biomechanics during two speeds of wheelchair propulsion: an analysis using local coordinate system. Arch Phys Med Rehab 1997;78:36472. Bonninger ML, Cooper RA, Baldwin MA, Shimada SD, Koontz AL. Wheelchair pushrim kinetics: body weight and median nerve conduction. Arch Phys Med Rehab 1999;80:9105. Veeger HEJ, van der Woude LHV. Fysiologische en mechanische belasting van rolstoelrijden. T v Fysiotherapie 1996;106(3):66 73 [in Dutch]. Veeger HEJ, Meershoek LS, van der Woude LHV, Langenhoff JM. Wrist motion in handrim wheelchair propulsion. J Rehab Res Dev 1998;35(3):30513. Boninger ML, Robertson RN, Wolff M, Cooper RA. Upper limb nerve entrapments in elite wheelchair racers. Am J Phys Med Rehab 1996;75:1706. Veeger HEJ, van der Woude LHV, Rozendaal RH. A computerized wheelchair ergometer: results of a comparison study. Scand J Rehab Med 1992;24(1):15864. van der Linden ML, Valent L, Veeger HEJ, van der Woude LHV. The effect of wheelchair handrim tube diameter on propulsion efciency and force application. IEEE Trans Rehab Eng 1996;4(3):12332. de Groot S, Boot CRL, van der Woude LHV, Veeger HEJ. Force application and gross mechanical efciency in handrim wheelchair propulsion. Med Sci Sports Exerc 2001, submitted for publication. Kofski PR, Davis GM, Shephard RJ, Jackson RW, Keene GC. Field testing: assessment of physical tness of disabled adults. Eur J Appl Phys 1983;51:10920. Wicks JR, Oldridge NB, Cameron BJ, Jones NL. Arm cranking and wheelchair ergometry in elite spinal cord-injured athletes. Med Sci Sports Exerc 1983;15:22431. Huonker M, Schmid A, Sorichter S, Schmidt-Trucksab A, Mrosek P, Keul J. Cardiovascular differences between sedentary and wheelchair-trained subjects with paraplegia. Med Sci Sports Exerc 1998;30(4):60913. Veeger HEJ, Hadj Yahmed M, van der Woude LHV, Charpentier P. Peak oxygen uptake and maximal power output of Olympic wheelchair-dependent athletes. Med Sci Sports Exerc 1991;23(10):12019. Janssen TWJ, van Oers CAJM, Hollander AP, Veeger HEJ, van der Woude LHV. Isometric strength, sprint power, and aerobic power in individuals with a spinal cord injury. Med Sci Sports Exerc 1993;25(7):86370. van der Woude LHV, Bakker WH, Elkhuizen JW, Veeger HE, Gwinn T. Anaerobic work capacity in elite wheelchair athletes. Am J Phys Med Rehab 1997;76(5):35565. Vanlandewijck YC, Spaepen AJ, Lysens RJ. Wheelchair propulsion efciency: movement pattern adaptations to speed changes. Med Sci Sports Exerc 1994;26(11):137381. Jacobs PL, Nash MS, Rusinowski JW. Circuit training provides cardiorespiratory and strength benets in persons with paraplegia. Med Sci Sports Exerc 2001;33(5):7117. Bednarczyk JH, Sanderson DJ. Kinematics of wheelchair propulsion in adults and children with spinal cord injury. Arch Phys Med Rehab 1994;75(12):132734. Sawka MN, Glaser RM, Laubach LL, Al-Samkari O, Suryaprasad AG. Wheelchair exercise performance of the young, middle-aged
732
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
and elderly. J Appl Physiol: Resp Environ Exerc Physiol 1981;50(4):8248. [89] Higgs C, Babstock P, Buck J, Parsons C, Brewer J. Wheelchair classication for track and eld events: a performance approach. Adapt Phys Act Quart 1990;7(1):2240. [90] Veeger, H.E.J., Woude, L.H.V.van der, Rozendal, R.H. (1991c) Within cycle characteristics of the wheelchair push in sprinting on a wheelchair ergometer Med Sci Sport Exerc 23, 264271. [91] Burnham RS, May L, Nelson E, Steadward RD, Reid DC. Shoulder pain in wheelchair athletes: the role of muscle imbalance. Am J Sports Med 1993;21(2):23842. [92] Burnham RS, Chan M, Hazlett C, Laskin J, Steadward RD. Acute median nerve dysfunction from wheelchair propulsion: the development of a model and study of the effect of hand protection. Arch Phys Med Rehab 1994;75:5138. [93] Curtis KA, Tyner TM, Zachary L, Lentell G, Brink D, Didyk T, Gean K, Hall J, Klos J, Lesina S, Pacillas B. Effect of a standard exercise protocol on shoulder pain in long-term wheelchair users. Spinal Cord 1999;37(6):4219. [94] Sie IH, Waters RL et al. Upper extremity pain in the postrehabilitation spinal cord patient. Arch Phys Med Rehabil 1992;73:448. [95] Subbarao JV, Klopfstein J. Prevalence and impact of wrist and shoulder pain in patients with spinal cord injury. J Spinal Cord Med 1995;18(1):913. [96] Wang YT, Deutsch H, Morse M, Hedrick B, Millikan T. Three dimensional kinematics of wheelchair propulsion across racing speeds. Adapt Phys Act Quart 1995;12:7889. [97] Burnham RS, Steadward RD. Upper extremity peripheral nerve entrapments among wheelchair athletes: prevalence, location and risk factors. Arch Phys Med Rehab 1994;75:51924. [98] Jackson DL, Hynninen BC, Caborn DN, McLean J. Electrodiagnostic study of carpal tunnel syndrome in wheelchair basketball players. Clin J Sport Med 1996;6(1):2731. [99] Roeleveld K, Lute E, Veeger HEJ, Gwinn T, van der Woude LHV. Power output and technique of wheelchair athletes. Adapt Phys Act Quart 1994;11(1):7185. [100] Veeger HEJ, Lute EM, Roeleveld K, van der Woude LHV. Differences in performance between trained and untrained subjects during a 30-s sprint test in a wheelchair ergometer. Eur J Appl Physiol Occup Physiol 1992;64(2):15864. [101] Veeger HEJ, van der Woude LHV. Force generation in manual wheelchair propulsion. In: XIII Southern Biomedical Engineering Conference, 1994:77982. [102] Campbell CC, Koris MJ. Etiologies of shoulder pain in cervical spinal cord injury. Clin Orthop Relat Res 1996;322:1405. [103] van der Woude LHV, Veeger HEJ, Rozendaal RH. Propulsion technique in hand rim wheelchair propulsion. J Med Eng Tech 1989;13(1):13641. [104] van der Helm FCT, Veeger HEJ et al. Analysis of the power balance during wheelchair propulsion using a 3-D musculoskeletal shoulder and elbow model. In: XVIth Congress of the International Society of Biomechanics. Tokyo: University of Tokyo, 1997. [105] van der Helm FCT, Veeger HEJ. Shoulder modelling in rehabilitation: the power balance during wheelchair propulsion. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:96103. [106] van der Helm FCT, Veeger HEJ. Quasi-static analysis of muscle forces in the shoulder mechanism during wheelchair propulsion. J Biomech 1996;29(1):3952. [107] Rozendaal LA, Veeger HEJ. Force direction in manual wheelchair propulsion: balance between cost and effect. Clin Biom 2000;15(suppl. 1):S3942. [108] Lafortune MA, Cavanagh PR. Effectiveness and efciency during bicycle riding. Biomechanics VII-B. Human Kinetics Publishers, 1983.
[109] Dallmeijer AJ, van der Woude LHV, Pathuis CS. Adaptations in wheelchair propulsion technique after training in able bodied subjects. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:2246. [110] Mulroy SJ, Gronley JK. Electromyographic activity of shoulder muscles during wheelchair propulsion by paraplegic persons. Arch Phys Med Rehab 1996;77:18793. [111] Veeger HEJ. Biomechanics of manual wheelchair propulsion. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:8696. [112] Dallmeijer AJ, van der Woude LHV, Veeger HEJ, Hollander AP. Effectiveness of force application in manual wheelchair propulsion in persons with spinal cord injuries. Am J Phys Med Rehab 1998;77(3):21321. [113] McLaurin CA. Determination of rolling resistance of manual wheelchairs. Thesis University of Virginia; 1983. [114] OReagan J, Thacker J, Kauzlarich J, Mochel E, Carmine D, Bryant M. Wheelchair dynamics. In: Wheelchair mobility 19761981. REC, University of Virginia, 1981:3341. [115] Weege RD. Technische Voraussetzungen fur den Aktivsport im Rollstuhl. Orthopaedie Technik 1985;36(6):395402. [116] Brubaker CE, McLaurin CA, McClay IS. Effects of side slope on wheelchair performance. J Rehab Res Dev 1986;23(2):558. [117] Abel EW, Frank TG. The design of attendant propelled wheelchairs. Prosthetics Orthotics Int 1991;15(1):3845. [118] Coe PL. Aerodynamic characteristics of wheelchairs (80191). NASA Technical Memorandum; 1979. [119] Hedrick B, Wang YT, Moeinzadeh M, Adrian M. Aerodynamics positioning and performance in wheelchair racing. Adapt Phys Act Quart 1990;7:4151. [120] Higgs C. Wheeling in the wind: the effect of wind velocity and direction on aerodynamic drag of wheelchairs. Adapt Phys Act Quart 1992;9:7487. [121] Whitt FR, Wilson DG. Bicycling science. London: MIT Press, 1982. [122] Bachl N, Ziegler JW, Baron R, Liebeberger S, Kirsten H, Prokop L. Verhaltern leistungsphysiologischer Parameter bei Rollstuhlfahrern unter Verwendung von verschiedene Uebersetzungsnaben zum Rollstuhlantrieb. Med Orthop Technik 1989;6:2358. [123] Engel P, Neikes M, Bennedik K, Hildebrandt G, Rode FW. Arbeitsphysiologische Untersuchungen zur Optimierung des Hebelantiebs und der Sitzanordnung. Med Orthop Technik 1976;98:2832. [124] Engel P, Hildebrandt G. Zur arbeitsphysiologische Beurteilung verschiedenen handbetriebenen Krankenfahrstuehlen. Zeitschrift fuer Physikalische Medizin 1971;2:95102. [125] van der Woude LHV, Veeger HE, De Boer Y, Rozendal RH. Physiological evaluation of a newly designed lever mechanism for wheelchairs. J Med Eng Tech 1993;17(6):23240. [126] Higgs C. An analysis of racing wheelchairs used at the 1980 Olympic Games for the Disabled. Res Quart Exerc Sport 1983;54(3):22933. [127] Davis GM, Shephard RJ. Cardiorespiratory tness in highly active versus inactive paraplegics. Med Sci Sports Exerc 1988;20(5):4638. [128] Gass EM, Harvey LA, Gass GC. Maximal physiological responses during arm cranking and treadmill wheelchair propulsion in T4T6 paraplegic men. Paraplegia 1995;33(5):26770. [129] Vinet A, Le Gallais D, Bernard PL, Poulain M, Varray A, Mercier J, Micallef JP. Aerobic metabolism and cardioventilatory responses in paraplegic athletes during incremental wheelchair exercise. Eur J Appl Phys 1997;76:45561. [130] Vanlandewijck YC, Spaepen AJ, Lysens RJ. Relationship between the level of physical impairment and sports perform-
L.H.V. van der Woude et al. / Medical Engineering & Physics 23 (2001) 713733
733
[131]
[132]
[133] [134]
[135]
ance in elite wheelchair basketball athletes. Adapt Phys Act Quart 1995;12:13950. Schmid A, Huonker M, Stober P, Barturen J-M, SchmidtTruckaess A, Duerr H, Voelpel H-A, Keul J. Physical performance and cardiovascular and metabolic adaptation of elite female wheelchair basketball players in wheelchair ergometry and in competition. Am J Phys Med Rehab 1998;77:52733. Coutts KD, Stogryn JL. Aerobic and anaerobic power of Canadian wheelchair track athletes. Med Sci Sports Exerc 1987;19(1):625. Lees A, Arthur S. An investigation into anaerobic performance of wheelchair athletes. Ergonomics 1988;31(11):152937. Hutzler Y, Ochana S, Bolotin R, Kalina E. Aerobic and anaerobic arm-cranking power outputs of males with lower limb impairments: relationship with sport participation intensity, age, impairment and functional classication. Spinal Cord 1998;36(3):20512. van der Woude LHV, Bakker WH, Elkhuizen JW, Veeger HEJ,
Gwinn T. Propulsion technique and anaerobic work capacity in elite wheelchair athletes: cross-sectional analysis. Am J Phys Med Rehab 1998;77(3):22234. [136] Dallmeijer AJ, Kappe YJ, Veeger HEJ, Janssen TW, van der Woude LHV. Anaerobic power output and propulsion technique in spinal cord injured subjects during wheelchair ergometry. J Rehab Res Dev 1994;31(2):1208. [137] van der Woude LHV, Guerts C, Winkelman H, Veeger HEJ. Measurement of rolling resistance with a push technique. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:1947. [138] Vlies FWJ, Gerritsma CJ, Veeger HEJ, van der Woude LHV. Physiological responses in hubcrank and handrim wheelchair propulsion using a computer controlled wheelchair ergometer. In: van der Woude LHV, Hopman MTE, van Kemenade C, editors. Biomedical aspects of manual wheelchair propulsion: state of the art II. Amsterdam: IOS Press, 1999:1904.
You might also like
- NAPLEX Prep 2018 Ch01 CardioDocument56 pagesNAPLEX Prep 2018 Ch01 CardioFaith50% (2)
- Assignment #3: Name: O'Neil Leitch USI: 1024833 Lecturer: Vishal Persaud Course Name: Research Method Course #: EMN 3202Document7 pagesAssignment #3: Name: O'Neil Leitch USI: 1024833 Lecturer: Vishal Persaud Course Name: Research Method Course #: EMN 3202leitchNo ratings yet
- Hindavi 5513013Document12 pagesHindavi 5513013Muthuvelan MutharasuNo ratings yet
- Design and Development of A Lightweight, High-Torque, and Cost-Effective Hip ExoskeletonDocument6 pagesDesign and Development of A Lightweight, High-Torque, and Cost-Effective Hip ExoskeletonSultan Mahi ZubairNo ratings yet
- Robotics: A Review On Design of Upper Limb ExoskeletonsDocument35 pagesRobotics: A Review On Design of Upper Limb ExoskeletonsDerekNo ratings yet
- Robotics: A Review On Design of Upper Limb ExoskeletonsDocument35 pagesRobotics: A Review On Design of Upper Limb ExoskeletonsCostinel BogheanuNo ratings yet
- Effeciency of HandpropulsionDocument159 pagesEffeciency of HandpropulsionJoshua MathewNo ratings yet
- Kinematic and Kinetic Functional RequirementsgDocument28 pagesKinematic and Kinetic Functional RequirementsgMabel PNo ratings yet
- Applied Sciences: Cycling Biomechanics and Its Relationship To PerformanceDocument15 pagesApplied Sciences: Cycling Biomechanics and Its Relationship To PerformanceMarcelo CarvalhoNo ratings yet
- Design of A Hip Joint Simulator According To The ISO 14242: Nikolaos I. Galanis, Member, IAENG and Dimitrios E. ManolakosDocument6 pagesDesign of A Hip Joint Simulator According To The ISO 14242: Nikolaos I. Galanis, Member, IAENG and Dimitrios E. ManolakosJosé santanaNo ratings yet
- Kinematic and Kinetic Functional Requirements For Industrial Exoskeletons For Lifting Tasks and Overhead LiftingDocument15 pagesKinematic and Kinetic Functional Requirements For Industrial Exoskeletons For Lifting Tasks and Overhead LiftingPulagam Lakshmi Sampath Reddy 21BME1298No ratings yet
- Medical Engineering and Physics: Nguiadem Clautilde, Raison Maxime, Achiche SofianeDocument10 pagesMedical Engineering and Physics: Nguiadem Clautilde, Raison Maxime, Achiche SofianeMatthew PhillipsNo ratings yet
- An Anthropometric Measurement For Developing PDFDocument17 pagesAn Anthropometric Measurement For Developing PDFAtharvaNo ratings yet
- A Review Study For Measurement, Analysis and Evaluation Four Bar Polycentric KneeDocument18 pagesA Review Study For Measurement, Analysis and Evaluation Four Bar Polycentric Kneejosephe.thrasherNo ratings yet
- A New Hand Exoskeleton Device For Rehabilitation Using A Three-Layered Sliding Spring Mechanism PDFDocument6 pagesA New Hand Exoskeleton Device For Rehabilitation Using A Three-Layered Sliding Spring Mechanism PDFGIenlemenNo ratings yet
- An Anthropometric Measurement For DeveloDocument17 pagesAn Anthropometric Measurement For DeveloPromit ChoudhuryNo ratings yet
- S12008-021-00779-9-Our RequirementDocument15 pagesS12008-021-00779-9-Our RequirementMuthuvelan MutharasuNo ratings yet
- Various Types of Wheel Chair ControlDocument6 pagesVarious Types of Wheel Chair ControlIAEME PublicationNo ratings yet
- Ergonomics, Biomechanics & Musculoskeletal Disorder-A ReviewDocument8 pagesErgonomics, Biomechanics & Musculoskeletal Disorder-A ReviewRenaldiPrimaSaputraNo ratings yet
- E039 PublishedDocument8 pagesE039 PublishedRenaldiPrimaSaputraNo ratings yet
- Prediction of Energy Efficient Pedal Forces in Cycling Using Musculoskeletal Simulation ModelsDocument5 pagesPrediction of Energy Efficient Pedal Forces in Cycling Using Musculoskeletal Simulation Modelsthe_answerNo ratings yet
- A New Controlling Parameter in Design of Above Knee ProsthesisDocument8 pagesA New Controlling Parameter in Design of Above Knee ProsthesismohsinslatchNo ratings yet
- Carney (2021)Document12 pagesCarney (2021)Fernanda LealNo ratings yet
- Analysis and Optimisation of All Terrain WheelchairDocument10 pagesAnalysis and Optimisation of All Terrain WheelchairAshish NandaNo ratings yet
- Engineering: Ronnapee Chaichaowarat, Jun Kinugawa, Kazuhiro KosugeDocument8 pagesEngineering: Ronnapee Chaichaowarat, Jun Kinugawa, Kazuhiro Kosugelaura bemudezNo ratings yet
- Exoskeleton Design For LegDocument8 pagesExoskeleton Design For LegGamini SureshNo ratings yet
- Prediction of Rowing Ergometer Performance by Technical and Core Stability Parameters-2Document10 pagesPrediction of Rowing Ergometer Performance by Technical and Core Stability Parameters-2strokeman75No ratings yet
- EnergyDocument13 pagesEnergyFernando BarónNo ratings yet
- Biomechanical Analysis of Electric Powered Wheelchair by Reverse Engineering Modelling TechnologyDocument9 pagesBiomechanical Analysis of Electric Powered Wheelchair by Reverse Engineering Modelling TechnologyDileep KumarNo ratings yet
- AbstractDocument28 pagesAbstractKetan MeshramNo ratings yet
- 1.0) Name 2.0) Project Title 3.0) Background:::: Design and Development of A Speech-Activated Bionic JointDocument6 pages1.0) Name 2.0) Project Title 3.0) Background:::: Design and Development of A Speech-Activated Bionic JointAhmed AbdulwahabNo ratings yet
- Applied SciencesDocument22 pagesApplied SciencesHamrah SiddiquiNo ratings yet
- Robot-Aided Neurorehabilitation: A Novel Robot For Ankle RehabilitationDocument15 pagesRobot-Aided Neurorehabilitation: A Novel Robot For Ankle RehabilitationabcNo ratings yet
- Design of A 7 Degree-of-Freedom Upper-Limb Powered ExoskeletonDocument6 pagesDesign of A 7 Degree-of-Freedom Upper-Limb Powered Exoskeletonfaizar_2No ratings yet
- CFD Simulations of The Aerodynamic Drag of Two Drafting CyclistsDocument17 pagesCFD Simulations of The Aerodynamic Drag of Two Drafting CyclistsmaorpeNo ratings yet
- Performance Assessment of A Pushrim-Activated Power-Assisted Wheelchair Control SystemDocument6 pagesPerformance Assessment of A Pushrim-Activated Power-Assisted Wheelchair Control SystemsdgNo ratings yet
- 1 s2.0 S1350453322000790 MainDocument8 pages1 s2.0 S1350453322000790 MainNANDHINIK 19BM059No ratings yet
- Mechanical Design of A Distal Arm Exoskeleton For Stroke and Spinal Cord Injury RehabilitationDocument5 pagesMechanical Design of A Distal Arm Exoskeleton For Stroke and Spinal Cord Injury RehabilitationOmar CirineoNo ratings yet
- Sensors: Estimating Human Wrist Stiffness During A Tooling TaskDocument14 pagesSensors: Estimating Human Wrist Stiffness During A Tooling TaskAdi CrişanNo ratings yet
- Electric Wheelchair Design and Its Impacts On Life Among The Disabled Individuals A ReviewDocument3 pagesElectric Wheelchair Design and Its Impacts On Life Among The Disabled Individuals A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Soft Elbow ExosuitDocument8 pagesA Novel Soft Elbow Exosuiteyao100% (1)
- Towards The Mechatronic Development of A New Upper-Limb Exoskeleton (SAMA)Document25 pagesTowards The Mechatronic Development of A New Upper-Limb Exoskeleton (SAMA)alamin khondakerNo ratings yet
- Micromachines 2544656 Peer Review v1Document21 pagesMicromachines 2544656 Peer Review v1Parvin AkterNo ratings yet
- Bio Kel IIIDocument5 pagesBio Kel IIIPerlin LimbongNo ratings yet
- LiteratureDocument8 pagesLiteraturebetelhemterefe wondimagenihuNo ratings yet
- Dynamic Optimization Design of Cranes Based On Human-Crane-Rail System Dynamics and Annoyance RateDocument19 pagesDynamic Optimization Design of Cranes Based On Human-Crane-Rail System Dynamics and Annoyance RateGogyNo ratings yet
- IJRPR23502Document4 pagesIJRPR23502Dharmaraj kisan KharpadeNo ratings yet
- Design of TreadmillDocument4 pagesDesign of Treadmillguest100% (1)
- Lovely Professional UniversityDocument4 pagesLovely Professional Universityshailesh_singh_19No ratings yet
- SFDSDFDocument13 pagesSFDSDFAkshhata NarulkarNo ratings yet
- Performance Characteristics of Anthropomorphic Prosthetic HandsDocument7 pagesPerformance Characteristics of Anthropomorphic Prosthetic HandsamirtempsNo ratings yet
- Design and Fabrication of Exoskeleton Arm For Lifting WeightDocument4 pagesDesign and Fabrication of Exoskeleton Arm For Lifting WeightIJRASETPublicationsNo ratings yet
- Effect of Hand Rim Diameter On Manual Wheelchair Propulsion Using Mechanical Energy and Power Flow AnalysisDocument9 pagesEffect of Hand Rim Diameter On Manual Wheelchair Propulsion Using Mechanical Energy and Power Flow AnalysisavalosheNo ratings yet
- Project Proposal-Robotic ProstheticdocxDocument6 pagesProject Proposal-Robotic ProstheticdocxAvk SanjeevanNo ratings yet
- Agonist-Antagonist Active Knee Prosthesis - A Preliminary Study in Level-Ground WalkingDocument13 pagesAgonist-Antagonist Active Knee Prosthesis - A Preliminary Study in Level-Ground Walkingrkp17No ratings yet
- Biomechanics Feedback For RowingDocument10 pagesBiomechanics Feedback For Rowingzé carlos batelNo ratings yet
- Elexo PDFDocument22 pagesElexo PDFPrince KumarNo ratings yet
- Discussion Paper: The Impact of Using Exoskeletons On Occupational Safety and HealthDocument10 pagesDiscussion Paper: The Impact of Using Exoskeletons On Occupational Safety and HealthFábioNo ratings yet
- Development of Four Bar MechanismDocument7 pagesDevelopment of Four Bar MechanismDbz BoleroNo ratings yet
- Recreational Mechanics: A Source Book for Walkers and Track CoachesFrom EverandRecreational Mechanics: A Source Book for Walkers and Track CoachesNo ratings yet
- NetScientific CMD Glucosense May 2015Document10 pagesNetScientific CMD Glucosense May 2015Stanislas AchardNo ratings yet
- Us 8267975Document14 pagesUs 8267975Stanislas AchardNo ratings yet
- Us 20120283630Document11 pagesUs 20120283630Stanislas AchardNo ratings yet
- United States Patent (19) (111 4,230,151: Jonsson (45) Oct. 28, 1980Document8 pagesUnited States Patent (19) (111 4,230,151: Jonsson (45) Oct. 28, 1980Stanislas AchardNo ratings yet
- Ep0339877a2 PDFDocument12 pagesEp0339877a2 PDFStanislas AchardNo ratings yet
- FDA Lead p960009 PDFDocument133 pagesFDA Lead p960009 PDFStanislas AchardNo ratings yet
- Us 6530231Document14 pagesUs 6530231Stanislas AchardNo ratings yet
- Document Summaries 1Document92 pagesDocument Summaries 1Stanislas AchardNo ratings yet
- 13 Areas of AssessmentDocument10 pages13 Areas of AssessmentNicole Anne TungolNo ratings yet
- HRV Clinical GuideDocument58 pagesHRV Clinical GuidePriscila LucaNo ratings yet
- The Five Best Brain StacksDocument33 pagesThe Five Best Brain StacksVishal Siguru100% (2)
- Mirror TracingDocument8 pagesMirror TracingMichael CamusNo ratings yet
- 11 Biology Notes ch18 Body Fluids and Circulation PDFDocument8 pages11 Biology Notes ch18 Body Fluids and Circulation PDFSumit SinghalNo ratings yet
- 100-Day Contract With Dairy CowDocument22 pages100-Day Contract With Dairy CowMarjorie SalgadoNo ratings yet
- CVDocument1 pageCVapi-377129715No ratings yet
- Gram Staining PDFDocument6 pagesGram Staining PDFMaria Chacón CarbajalNo ratings yet
- Recent Advances in HypertensionDocument6 pagesRecent Advances in Hypertensionrudi saputraNo ratings yet
- HypothermiaDocument9 pagesHypothermiaRieskyDwiUtomoNo ratings yet
- Minerals Sports Club November Fitness ScheduleDocument2 pagesMinerals Sports Club November Fitness ScheduleMineralsSportsClubNo ratings yet
- Neuroplasticity and NeurorehabilitationDocument164 pagesNeuroplasticity and Neurorehabilitationn0rbertt0% (1)
- Brain Gym ExercisesDocument9 pagesBrain Gym ExercisesMuza RasidiNo ratings yet
- Clayton & Willihnganz: Basic Pharmacology For Nurses, 17th EditionDocument4 pagesClayton & Willihnganz: Basic Pharmacology For Nurses, 17th EditionabsianoNo ratings yet
- Mani Dweepa Varnana in TeluguDocument165 pagesMani Dweepa Varnana in Telugukngane8878100% (4)
- Biology Notes: Cie IgcseDocument64 pagesBiology Notes: Cie Igcsehamza96No ratings yet
- The Essential Qigong TrainingDocument32 pagesThe Essential Qigong TrainingSoumen100% (1)
- Experiment 1 Cell BioDocument7 pagesExperiment 1 Cell BioWinserng 永森No ratings yet
- AB BC : Part ADocument39 pagesAB BC : Part AApoorva GuptaNo ratings yet
- Confidence Cheat Sheet: Matt ArtisanDocument40 pagesConfidence Cheat Sheet: Matt ArtisanAbhijit BanikNo ratings yet
- BT1001 Biology For Engineers PDFDocument2 pagesBT1001 Biology For Engineers PDFsanthi saranyaNo ratings yet
- Qatar - Blueprint and Reference (Dec 2016)Document7 pagesQatar - Blueprint and Reference (Dec 2016)Jashim Jumli IINo ratings yet
- Case Pres NCP ProperDocument3 pagesCase Pres NCP ProperMyraNo ratings yet
- Principles of Vegetative PropagationDocument5 pagesPrinciples of Vegetative PropagationJensenNo ratings yet
- The Brain Has A Body Adaptive Behavior Emerges From Interactions of Nervous System, Body and Environment by Hillel J. Chiel and Randall D. Beer 1997Document5 pagesThe Brain Has A Body Adaptive Behavior Emerges From Interactions of Nervous System, Body and Environment by Hillel J. Chiel and Randall D. Beer 1997AmiraNo ratings yet
- Pelvic Organ ProlapseDocument68 pagesPelvic Organ ProlapseAlyanna CrisologoNo ratings yet
- Qrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument49 pagesQrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramMuhammad Hatta HamzahNo ratings yet
- Science 8 Fourth 4 DaysDocument4 pagesScience 8 Fourth 4 DaysAshley Lopez100% (5)
- Spinal Cord Injury NotesDocument13 pagesSpinal Cord Injury Notescorememories10No ratings yet