You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Doxazosin Mesilate - Martindale 36edDocument1 pageDoxazosin Mesilate - Martindale 36edSvetlana Maiochi LodovicoNo ratings yet
- T1K UpdateDocument24 pagesT1K UpdateolivenanaNo ratings yet
- Colorado Guidelines of Professional Practice For Controlled SubstancesDocument65 pagesColorado Guidelines of Professional Practice For Controlled SubstancesBrian HarrisNo ratings yet
- List of Drug Manufacturers Recognized for ExcellenceDocument2 pagesList of Drug Manufacturers Recognized for Excellencechowder_coronado67% (18)
- Test Farma En-Ro, Ro-EnDocument3 pagesTest Farma En-Ro, Ro-EnIuliaUngurNo ratings yet
- Sinatra ReferenceDocument7 pagesSinatra ReferenceNavisa HaifaNo ratings yet
- BARCODESDocument7 pagesBARCODESChitPerRhosNo ratings yet
- Metoclopramide and Rosuvastatin Nursing ConsiderationsDocument5 pagesMetoclopramide and Rosuvastatin Nursing ConsiderationsDianne NemisNo ratings yet
- Nebu&CPTDocument32 pagesNebu&CPTAbigail Bantayan100% (1)
- The Association Between Stage of Treatment Resistant Depression and Clinical Utility of KetamineesketamineDocument48 pagesThe Association Between Stage of Treatment Resistant Depression and Clinical Utility of KetamineesketamineArgenis SalinasNo ratings yet
- Library G.Pulla Reddy College of Pharmacy Hyderabad: OU - 1705 OU - 1705Document10 pagesLibrary G.Pulla Reddy College of Pharmacy Hyderabad: OU - 1705 OU - 1705A.vidhyavandhanareddyNo ratings yet
- Prescribing Authority TableDocument7 pagesPrescribing Authority TablearifadamjiNo ratings yet
- Curriculum Vitae MTDocument6 pagesCurriculum Vitae MTapi-273097827No ratings yet
- Exotic Hypnosis Inductions - Unusual & Unique Hypnosis TechniquesDocument3 pagesExotic Hypnosis Inductions - Unusual & Unique Hypnosis Techniquesgmeades33% (3)
- Debridement of Large WoundsDocument1 pageDebridement of Large WoundsMeddco helpdeskNo ratings yet
- PPM Arvreferencepricing Table enDocument3 pagesPPM Arvreferencepricing Table enayawe888888No ratings yet
- Review 1. Efficacy and Safety of Cetuximab For CRCDocument13 pagesReview 1. Efficacy and Safety of Cetuximab For CRCcollianairaNo ratings yet
- Cebu Normal University College of Nursing Drug StudyDocument5 pagesCebu Normal University College of Nursing Drug StudyFaye Andrea Francisco100% (1)
- List Harga Quantum UpdateDocument1 pageList Harga Quantum UpdateAde IrawanNo ratings yet
- MMP Handy Chart October 2011 V2Document37 pagesMMP Handy Chart October 2011 V2ColonNo ratings yet
- Netupitant & PalonosetronDocument2 pagesNetupitant & PalonosetronShamim Ahamed ShakilNo ratings yet
- Ventilator The Basic CourseDocument117 pagesVentilator The Basic CourseTputrinya FaniddaNo ratings yet
- 21 AdisaDocument6 pages21 AdisaTri UtariNo ratings yet
- Off-Label Drug Use in Pediatric Patients: ReviewsDocument6 pagesOff-Label Drug Use in Pediatric Patients: ReviewsRestu SNo ratings yet
- Smu066 PDF EngDocument9 pagesSmu066 PDF EngDEREK SANDOVALNo ratings yet
- ΔΤΦ 06082013Document1,140 pagesΔΤΦ 06082013LOUI_GRNo ratings yet
- Telemetry-Intermediate Care Skills ChecklistDocument4 pagesTelemetry-Intermediate Care Skills ChecklistnorthweststaffingNo ratings yet
- 1 PBDocument14 pages1 PBindah marhaniNo ratings yet
- The Morphine Manifesto 2023Document6 pagesThe Morphine Manifesto 2023Fatul Chelseakers ZhinZhaiNo ratings yet
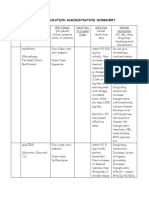
- Medication Administration WorksheetDocument6 pagesMedication Administration WorksheetCheska CarrionNo ratings yet