You might also like
- Sebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- MainDocument11 pagesMainMuhammad Nur Ardhi LahabuNo ratings yet
- Conway Lien, MD Mahesh R Patel, MDDocument8 pagesConway Lien, MD Mahesh R Patel, MDBoby SuryawanNo ratings yet
- Dermoid CystDocument8 pagesDermoid CystBoby SuryawanNo ratings yet
- Dermo IdDocument5 pagesDermo IdJohn Christopher LucesNo ratings yet
- 101-Normal Skin MCQsDocument25 pages101-Normal Skin MCQsHybat ElsheikhNo ratings yet
- Dermoid Cyst-Grand RoundsDocument13 pagesDermoid Cyst-Grand RoundsjojolilimomoNo ratings yet
- Dermoid CystDocument8 pagesDermoid CystMohamed Hazem ElfollNo ratings yet
- Milia PaperDocument14 pagesMilia PaperWito Eka PutraNo ratings yet
- Dermoid CystDocument29 pagesDermoid CystAlik ChuaNo ratings yet
- Benignskinlesions 141227191914 Conversion Gate01 PDFDocument109 pagesBenignskinlesions 141227191914 Conversion Gate01 PDFrinaldy IX9No ratings yet
- Benign Skin LesionsDocument109 pagesBenign Skin Lesionsrinaldy IX9No ratings yet
- Dermal CylindromaDocument4 pagesDermal CylindromaDeba P SarmaNo ratings yet
- An Unusual Eyelid Mass: Tarsal Dermoid Cyst: Case ReportDocument3 pagesAn Unusual Eyelid Mass: Tarsal Dermoid Cyst: Case ReportRicarhdo Valentino HanafiNo ratings yet
- A) Anatomi Dan Histologi Kulit Kepala / Scalp ? JawabDocument11 pagesA) Anatomi Dan Histologi Kulit Kepala / Scalp ? JawabMahesa NasutionNo ratings yet
- SKIN Tumors With Apocrine DifferentiationDocument101 pagesSKIN Tumors With Apocrine DifferentiationchinnnababuNo ratings yet
- CASE Report Basal Cell Carsinoma of NoseDocument22 pagesCASE Report Basal Cell Carsinoma of NoseDestar Aditya SadegaNo ratings yet
- Nose Basal Cell CarcinomaDocument24 pagesNose Basal Cell CarcinomadianNo ratings yet
- Dermoid CystDocument4 pagesDermoid Cystmicheal1960No ratings yet
- Neck Swellings (Compatibility Mode)Document49 pagesNeck Swellings (Compatibility Mode)vihang146No ratings yet
- IndianJOphthalmol643177-2181389 060333Document14 pagesIndianJOphthalmol643177-2181389 060333Zanty Rakhmania PutriNo ratings yet
- SEMINAR On Eyelid Echi 3rd YearDocument93 pagesSEMINAR On Eyelid Echi 3rd Yearsushmitabiswas052No ratings yet
- 7.5 Minor Surgical Conditions of ChildhoodDocument13 pages7.5 Minor Surgical Conditions of ChildhoodΜατθαίος ΠαππάςNo ratings yet
- Limbal DermoidDocument4 pagesLimbal DermoidPranjali ChhayaNo ratings yet
- Periorbital Dermoid Cyst PDFDocument3 pagesPeriorbital Dermoid Cyst PDFRicarhdo Valentino HanafiNo ratings yet
- Oral Pathology: Non-Epithelialized Primary Bone CystDocument4 pagesOral Pathology: Non-Epithelialized Primary Bone Cystعلي صادق جعفرNo ratings yet
- Dermoid Cyst - StatPearls - NCBI BookshelfDocument7 pagesDermoid Cyst - StatPearls - NCBI BookshelfAbdullahi nurudeenNo ratings yet
- Differential Diagnosis of A Neck Mass - UpToDateDocument16 pagesDifferential Diagnosis of A Neck Mass - UpToDatezzellowknifeNo ratings yet
- Differential Diagnosis of A Neck Mass - UpToDate PDFDocument16 pagesDifferential Diagnosis of A Neck Mass - UpToDate PDFDr.Anurag FursuleNo ratings yet
- Branchial Cleft CystDocument6 pagesBranchial Cleft CystIvana SupitNo ratings yet
- Excision of Branchial Cleft CystsDocument10 pagesExcision of Branchial Cleft Cystssjs315No ratings yet
- Ameloblastoma 140624025211 Phpapp02Document51 pagesAmeloblastoma 140624025211 Phpapp02agusNo ratings yet
- Leg, Arm, and Chest Papules: ERM ASEDocument9 pagesLeg, Arm, and Chest Papules: ERM ASEdeenutz93No ratings yet
- Dermatopathology Quiz 2.Document13 pagesDermatopathology Quiz 2.Deba P SarmaNo ratings yet
- Microtia TaufiqDocument13 pagesMicrotia TaufiqAldy BimaNo ratings yet
- Dermoid Cyst: Jump To Navigation Jump To SearchDocument4 pagesDermoid Cyst: Jump To Navigation Jump To Searchfgfxgx100% (1)
- Background: Muir-Torre SyndromeDocument11 pagesBackground: Muir-Torre Syndromeadela_97lineNo ratings yet
- Skin LesionDocument23 pagesSkin Lesion5alifa55No ratings yet
- Sweat Gland TumorDocument3 pagesSweat Gland TumorM Azeneth JJNo ratings yet
- Keloids: Clinica L Fea Tures A ND M A Na Gem Ent.: Review ArticleDocument8 pagesKeloids: Clinica L Fea Tures A ND M A Na Gem Ent.: Review ArticleAndri Feisal NasutionNo ratings yet
- Cholesteatoma, An Overview May 2013Document9 pagesCholesteatoma, An Overview May 2013syukrinaalviNo ratings yet
- Maxillofacial DermoidDocument16 pagesMaxillofacial Dermoidj7mxqbhntcNo ratings yet
- Seborrheic KeratosisDocument12 pagesSeborrheic KeratosisMaiza MujadillahNo ratings yet
- v10 Literature Review Auricular Disorders Part 2 - Benign NeoplasmsDocument5 pagesv10 Literature Review Auricular Disorders Part 2 - Benign NeoplasmsAlisNo ratings yet
- Keratosis Obturans Is Commonly Associated WithDocument11 pagesKeratosis Obturans Is Commonly Associated WithAbouzr Mohammed ElsaidNo ratings yet
- باثوو برزنتيشنDocument40 pagesباثوو برزنتيشنLojin HaddadNo ratings yet
- CylindromaDocument1 pageCylindromaDeba P SarmaNo ratings yet
- Development of Integumentary Sytem With AudioDocument36 pagesDevelopment of Integumentary Sytem With AudioRetrocasualty Find OutNo ratings yet
- Oral Pathology Lec - 1Document11 pagesOral Pathology Lec - 1مصطفى محمدNo ratings yet
- Department of Prasuti Tantra and Striroga Dayanand Ayurvedic College, Jalandhar SESSION 2016-17Document40 pagesDepartment of Prasuti Tantra and Striroga Dayanand Ayurvedic College, Jalandhar SESSION 2016-17jyothiNo ratings yet
- Neck Mass ProtocolDocument8 pagesNeck Mass ProtocolCharlene FernándezNo ratings yet
- CH 04Document25 pagesCH 04tanvi vijayNo ratings yet
- Ostrower Preauricular Cysts, Pits, and Fissures - Practice Essentials, Epidemiology, EtiologyDocument8 pagesOstrower Preauricular Cysts, Pits, and Fissures - Practice Essentials, Epidemiology, EtiologyAndre HawkNo ratings yet
- Stevens-Johnson Syndrome CASEDocument38 pagesStevens-Johnson Syndrome CASEChristy Rose AgrisNo ratings yet
- Lecturenote - 819851336surgery of Head and NeckDocument16 pagesLecturenote - 819851336surgery of Head and NeckNuur AddiinNo ratings yet
- Appendigeal TumoursDocument3 pagesAppendigeal TumourspritanuNo ratings yet
- Aruns PL - Ade FinalDocument9 pagesAruns PL - Ade FinaldrarunsinghNo ratings yet
- MRCPCH - Important Skin DiseasesDocument42 pagesMRCPCH - Important Skin DiseasesarjumandNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
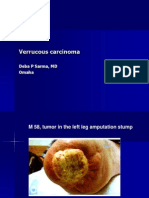
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
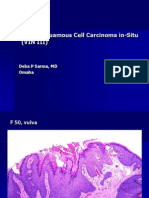
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Functional Dyspepsia in Adults PDFDocument15 pagesFunctional Dyspepsia in Adults PDFOdivan de CostaNo ratings yet
- Knee Pain With Possible Torn MeniscusDocument2 pagesKnee Pain With Possible Torn MeniscusHugh Ell - auNo ratings yet
- Medication Competency Questions For NursesDocument13 pagesMedication Competency Questions For NursesAlex AndrewNo ratings yet
- Malaria in Pregnancy. NewDocument23 pagesMalaria in Pregnancy. Newgloriashirima8No ratings yet
- Iron SucroseDocument3 pagesIron SucroseAtul KumarNo ratings yet
- MCQ EpiDocument45 pagesMCQ Episergioprofessor9860No ratings yet
- Haemaroids CaseDocument11 pagesHaemaroids CaseYugesvari_Thir_1690No ratings yet
- Kumpulan Diagnosas Klinik/poliklinikDocument10 pagesKumpulan Diagnosas Klinik/poliklinikHadiyasa JatmikaNo ratings yet
- Colonic Carcinoma Case StudyDocument23 pagesColonic Carcinoma Case StudyGlaiza Claire Am-amlan OlayanNo ratings yet
- Debridat CT 9409Document9 pagesDebridat CT 9409Mey KhNo ratings yet
- E100222 FullDocument7 pagesE100222 FullIki IdriansyahNo ratings yet
- Gastrointestinal Quiz AnswersDocument5 pagesGastrointestinal Quiz AnswersFranciskhokhyx III100% (5)
- BoardDocument20 pagesBoardJhecyn Marie PopiocoNo ratings yet
- Management of Ludwig's AnginaDocument13 pagesManagement of Ludwig's AnginaNahal HashirNo ratings yet
- Physical Diagnosis of The ThoraxDocument3 pagesPhysical Diagnosis of The ThoraxSeff Causapin100% (1)
- Basic Concepts of Pathology and PathophysiologyDocument10 pagesBasic Concepts of Pathology and PathophysiologyIra Agustyne DamanikNo ratings yet
- 3, Annex-3, Tables-13 A and B, 2018-19Document6 pages3, Annex-3, Tables-13 A and B, 2018-19Sumit BiswasNo ratings yet
- PenileDocument2 pagesPenileAREOLA Vera SophiaNo ratings yet
- NCP - BedriddenDocument4 pagesNCP - Bedriddenadelaigner_racho589475% (4)
- NCM 112 Care of Clients With ProblemsDocument3 pagesNCM 112 Care of Clients With Problems2C - Michaela Shenna DelfinNo ratings yet
- ECSTACY Final ReportingDocument15 pagesECSTACY Final ReportingCHRISTIAN RAY ALPAS PASILIAONo ratings yet
- Kertas Kerja PinjamanDocument18 pagesKertas Kerja PinjamanWan AzmanNo ratings yet
- Edited Insecticidal Efficacy and Repellency of OreganoDocument9 pagesEdited Insecticidal Efficacy and Repellency of OreganoChu Gabriel100% (1)
- Oral PathologyDocument31 pagesOral PathologyAnonymous GyqTkXMwMNo ratings yet
- Seyfert 2009Document6 pagesSeyfert 2009yane sofNo ratings yet
- Aaa Gastrectomy NCP FinalDocument13 pagesAaa Gastrectomy NCP Finallexzaf100% (1)
- Clinical Manifestations and Diagnosis of Urinary Tract Obstruction and Hydroneph PDFDocument32 pagesClinical Manifestations and Diagnosis of Urinary Tract Obstruction and Hydroneph PDFAmjad Saud0% (1)
- Hubungan Pengetahuan Dan Sikap Ibu Dengan Kejadian Diare Pada Balita Di Wilayah Kerja Puskesmas Punti Kayu PalembangDocument8 pagesHubungan Pengetahuan Dan Sikap Ibu Dengan Kejadian Diare Pada Balita Di Wilayah Kerja Puskesmas Punti Kayu PalembangAnisa SafutriNo ratings yet
- Script For Gradderall XVDocument4 pagesScript For Gradderall XVapi-273399286No ratings yet
- The COC Protocol™ in Pancreatic Cancer - Care Oncology USDocument14 pagesThe COC Protocol™ in Pancreatic Cancer - Care Oncology USStep T.No ratings yet