You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Application of Erich Arch BarDocument23 pagesApplication of Erich Arch BarDennis Andrew RemigioNo ratings yet
- GenTorque Con VB6 CODE PDFDocument518 pagesGenTorque Con VB6 CODE PDFhfalanizNo ratings yet
- 05.12 Anatomy of The Larynx & Physiology of PhonationDocument30 pages05.12 Anatomy of The Larynx & Physiology of PhonationReg LagartejaNo ratings yet
- (K24) Acute & Chronic LaryngitisDocument47 pages(K24) Acute & Chronic LaryngitisSyarifah Fauziah100% (3)
- Mastoidectomy VS Tympanoplasty - A Conceptual Renaissance. Preamble To An Original Method of Mastoidectom PDFDocument5 pagesMastoidectomy VS Tympanoplasty - A Conceptual Renaissance. Preamble To An Original Method of Mastoidectom PDFPutu Reza Sandhya PratamaNo ratings yet
- Haircuts Just Above Your Shoulders - Google SearchDocument1 pageHaircuts Just Above Your Shoulders - Google SearchBrynnleigh SmithNo ratings yet
- Radioimagistica SNC LP Stud 2020Document108 pagesRadioimagistica SNC LP Stud 2020MosiwiNo ratings yet
- Lecture Notes in Anatomy Embryology of The Oral CavityDocument9 pagesLecture Notes in Anatomy Embryology of The Oral Cavitykasonde bowaNo ratings yet
- The Eight Components of A Balanced SmileDocument17 pagesThe Eight Components of A Balanced SmileJose AriasNo ratings yet
- Thyroid ReportDocument31 pagesThyroid ReportMarion PerniaNo ratings yet
- Anatomy of The EyesDocument2 pagesAnatomy of The EyesTricia De TorresNo ratings yet
- CAP Protocol-2016 Larynx - HighlightedDocument7 pagesCAP Protocol-2016 Larynx - Highlightedpath2016No ratings yet
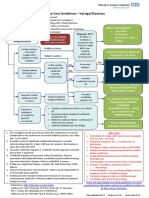
- ENT Vertigo FINAL v0.41Document1 pageENT Vertigo FINAL v0.41Farmasi BhamadaNo ratings yet
- Treatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceDocument9 pagesTreatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceJuan Carlos MeloNo ratings yet
- Appearance VocabularyDocument2 pagesAppearance VocabularyagaNo ratings yet
- The Diagnosis and Management ofDocument3 pagesThe Diagnosis and Management ofPreetam PatnalaNo ratings yet
- Circle WillisDocument42 pagesCircle WillisShazada KhanNo ratings yet
- Approaches To Frontal SinusDocument77 pagesApproaches To Frontal SinusHossam Elden Helmy HaridyNo ratings yet
- Ent PPT On Pharyngeal AbscessDocument20 pagesEnt PPT On Pharyngeal AbscessDocwocNo ratings yet
- First Periodical Test Science and Health 3Document4 pagesFirst Periodical Test Science and Health 3Bianca Camille Quiazon AguilusNo ratings yet
- Unlocking Orthodontic Malocclusions An Interplay Betw - 1998 - Seminars in OrthDocument10 pagesUnlocking Orthodontic Malocclusions An Interplay Betw - 1998 - Seminars in OrthmikeekimNo ratings yet
- Ent Imp Points To Diagnose ScenariosDocument46 pagesEnt Imp Points To Diagnose Scenariosusmandumassar0% (1)
- AnemiaDocument9 pagesAnemiaManjeevNo ratings yet
- Submental Artery Island Flap Technique For Head Neck ReconstructionDocument18 pagesSubmental Artery Island Flap Technique For Head Neck ReconstructionMahir NuredinNo ratings yet
- Anterior Clinoidectomy Using An Extradural and Intradural 2-Step Hybrid TechniqueDocument10 pagesAnterior Clinoidectomy Using An Extradural and Intradural 2-Step Hybrid TechniquekushalNo ratings yet
- Human hair experiment characteristics under SEMDocument2 pagesHuman hair experiment characteristics under SEMAngielenNo ratings yet
- MnemonicsDocument11 pagesMnemonicsanon-626602No ratings yet
- Soft Tissue Analysis: Dr. Ayushi Toley PG Ist YearDocument70 pagesSoft Tissue Analysis: Dr. Ayushi Toley PG Ist YearAyushi ToleyNo ratings yet
- Maxillofacial Trauma Le Fort 2Document120 pagesMaxillofacial Trauma Le Fort 2Irene UdarbeNo ratings yet
- Foreign Bodies in OtolaryngologyDocument31 pagesForeign Bodies in OtolaryngologyTarek Abdel FattahNo ratings yet