You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- (Brendan Brown) What Drives Global Capital FlowsDocument275 pages(Brendan Brown) What Drives Global Capital FlowserereredssdfsfdsfNo ratings yet
- Yamaha Piano Contract DisputeDocument11 pagesYamaha Piano Contract DisputeGalvin ChongNo ratings yet
- SDL Researchers Nominated For Prestigious European Inventor Award and Recognized For Creating A New MarketDocument2 pagesSDL Researchers Nominated For Prestigious European Inventor Award and Recognized For Creating A New MarketSDL Language TechnologiesNo ratings yet
- EXFO Selects SDL To Shorten Global Product Launch CyclesDocument2 pagesEXFO Selects SDL To Shorten Global Product Launch CyclesSDL Language TechnologiesNo ratings yet
- SDL Powers Global Translational Services For HusqvarnaDocument2 pagesSDL Powers Global Translational Services For HusqvarnaSDL Language TechnologiesNo ratings yet
- SDL PLC Q1 Interim Management StatementDocument2 pagesSDL PLC Q1 Interim Management StatementSDL Language TechnologiesNo ratings yet
- Benefits of Government Translation SolutionsDocument1 pageBenefits of Government Translation SolutionsSDL Language TechnologiesNo ratings yet
- SDL Helps U.S. Pharmacopeial Convention Optimize Customer ExperienceDocument2 pagesSDL Helps U.S. Pharmacopeial Convention Optimize Customer ExperienceSDL Language TechnologiesNo ratings yet
- United Kingdom Announces Revised Timetable To Implement Employment Law Reforms - International HR Services TeamDocument2 pagesUnited Kingdom Announces Revised Timetable To Implement Employment Law Reforms - International HR Services TeamSDL Language TechnologiesNo ratings yet
- SDL Appoints Grant Johnson As Chief Marketing OfficerDocument2 pagesSDL Appoints Grant Johnson As Chief Marketing OfficerSDL Language TechnologiesNo ratings yet
- SDL Receives Silver Winner Great Mind Award From The Advertising Research FoundationDocument2 pagesSDL Receives Silver Winner Great Mind Award From The Advertising Research FoundationSDL Language TechnologiesNo ratings yet
- Preliminary Results For The Year Ended 31 December 2012Document3 pagesPreliminary Results For The Year Ended 31 December 2012SDL Language TechnologiesNo ratings yet
- Hong Kong: Amendments To Direct Marketing Privacy Ordinance Effective From April 1, 2013Document2 pagesHong Kong: Amendments To Direct Marketing Privacy Ordinance Effective From April 1, 2013SDL Language TechnologiesNo ratings yet
- Whitepaper - Optimizing Multilingual Labeling ProcessesDocument13 pagesWhitepaper - Optimizing Multilingual Labeling ProcessesSDL Language TechnologiesNo ratings yet
- SDL Accelerates Customer Experience Management Initiatives With New Release of Web Content Management TechnologyDocument2 pagesSDL Accelerates Customer Experience Management Initiatives With New Release of Web Content Management TechnologySDL Language TechnologiesNo ratings yet
- SDL Named One of The 100 Companies That Matter in Knowledge ManagementDocument2 pagesSDL Named One of The 100 Companies That Matter in Knowledge ManagementSDL Language TechnologiesNo ratings yet
- SDL To Supply Multiple European Union Institutions With Computer-Aided Translation SolutionsDocument2 pagesSDL To Supply Multiple European Union Institutions With Computer-Aided Translation SolutionsSDL Language TechnologiesNo ratings yet
- Why Should You Invest in An Automated Translation SoftwareDocument1 pageWhy Should You Invest in An Automated Translation SoftwareSDL Language TechnologiesNo ratings yet
- SDL Announces Sponsorship of Translators Without BordersDocument2 pagesSDL Announces Sponsorship of Translators Without BordersSDL Language TechnologiesNo ratings yet
- Whitepaper - Optimizing Multilingual Labeling ProcessesDocument13 pagesWhitepaper - Optimizing Multilingual Labeling ProcessesSDL Language TechnologiesNo ratings yet
- Case Study - NexentaDocument2 pagesCase Study - NexentaSDL Language TechnologiesNo ratings yet
- Whitepaper - How Financial Institutions Use Live ChatDocument14 pagesWhitepaper - How Financial Institutions Use Live ChatSDL Language TechnologiesNo ratings yet
- Whitepaper - Applying Language Technology To Multilingual LabelingDocument8 pagesWhitepaper - Applying Language Technology To Multilingual LabelingSDL Language TechnologiesNo ratings yet
- SDL Announces The Opening of Elevation Center - The Localization Industry's First Briefing Center For Cloud ComputingDocument2 pagesSDL Announces The Opening of Elevation Center - The Localization Industry's First Briefing Center For Cloud ComputingSDL Language TechnologiesNo ratings yet
- SDL GlobalConnect 3.0 Delivers Integration With SDL BeGlobalDocument2 pagesSDL GlobalConnect 3.0 Delivers Integration With SDL BeGlobalSDL Language TechnologiesNo ratings yet
- SDL Proud Winner of 2011 International Business AwardDocument2 pagesSDL Proud Winner of 2011 International Business AwardSDL Language TechnologiesNo ratings yet
- SDL Automated Translation Solutions Give Government Organizations Timely Access To Mission-Critical InformationDocument2 pagesSDL Automated Translation Solutions Give Government Organizations Timely Access To Mission-Critical InformationSDL Language TechnologiesNo ratings yet
- 3.time Value of Money..F.MDocument21 pages3.time Value of Money..F.MMarl MwegiNo ratings yet
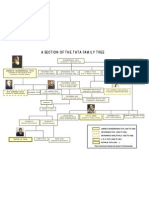
- TATA Family TreeDocument1 pageTATA Family Treemehulchauhan_9950% (2)
- Top US Companies by RegionDocument88 pagesTop US Companies by RegionLalith NeeleeNo ratings yet
- MAN Machine Material: Bottle Dented Too MuchDocument8 pagesMAN Machine Material: Bottle Dented Too Muchwaranya suttiwanNo ratings yet
- MCR2E Chapter 1 SlidesDocument14 pagesMCR2E Chapter 1 SlidesRowan RodriguesNo ratings yet
- Str. Poieni Nr. 1 Wernersholmvegen 5 5232 Paradis NORWAY: Seatrans Crewing A/S Constanta Filip, Dumitru IulianDocument1 pageStr. Poieni Nr. 1 Wernersholmvegen 5 5232 Paradis NORWAY: Seatrans Crewing A/S Constanta Filip, Dumitru Iuliandumitru68No ratings yet
- Corporate Governance Assignment by JunaidDocument3 pagesCorporate Governance Assignment by JunaidTanzeel HassanNo ratings yet
- PSP Study Guide 224 Q & A Revision Answers OlnyDocument214 pagesPSP Study Guide 224 Q & A Revision Answers OlnyMohyuddin A Maroof100% (1)
- IBS Renault Nissan Alliance FinalDocument24 pagesIBS Renault Nissan Alliance FinalakshaykgNo ratings yet
- CH 09Document35 pagesCH 09ReneeNo ratings yet
- Dwnload Full Retailing 8th Edition Dunne Test Bank PDFDocument35 pagesDwnload Full Retailing 8th Edition Dunne Test Bank PDFjayden4r4xarnold100% (14)
- Reading For The Real World - 2nd - AK - 3Document24 pagesReading For The Real World - 2nd - AK - 3vanthuannguyenNo ratings yet
- Arizona Exemptions 7-20-11Document1 pageArizona Exemptions 7-20-11DDrain5376No ratings yet
- Recommendations For TOWSDocument9 pagesRecommendations For TOWSShahzad KhanNo ratings yet
- Mandatory Disclosure2Document51 pagesMandatory Disclosure2prem chand tiwariNo ratings yet
- Customer preferences drive mobile choicesDocument12 pagesCustomer preferences drive mobile choicesNeha Kanak100% (2)
- Basel III Capital Regulations and Liquidity StandardsDocument40 pagesBasel III Capital Regulations and Liquidity Standardsrodney101No ratings yet
- Credit Managment of United Commercial Bank LimitedDocument54 pagesCredit Managment of United Commercial Bank LimitedMethela Barua100% (3)
- Project On SpicesDocument96 pagesProject On Spicesamitmanisha50% (6)
- Steel Prospectus in GCCDocument4 pagesSteel Prospectus in GCCAshish AggarwalNo ratings yet
- Impact of LiberalisationDocument23 pagesImpact of Liberalisationsourabhverdia100% (5)
- Security agency cost report for NCRDocument25 pagesSecurity agency cost report for NCRRicardo DelacruzNo ratings yet
- Bir Ruling Da 192-08Document2 pagesBir Ruling Da 192-08norliza albutraNo ratings yet
- 07 Bim PXP Guide-V2.0Document126 pages07 Bim PXP Guide-V2.0Felix Maurelio Canchari MallquiNo ratings yet
- AR JBN JANUARY 03 and JANUARY 10, 2023Document1 pageAR JBN JANUARY 03 and JANUARY 10, 2023h3ro007No ratings yet
- Find the perfect candidate for Wakil Kepala Klinik Utama GR Setra CMIDocument2 pagesFind the perfect candidate for Wakil Kepala Klinik Utama GR Setra CMIRscmi Dan LaboratoriumNo ratings yet
- North America Equity ResearchDocument8 pagesNorth America Equity ResearchshamashmNo ratings yet
- Hrmsr83pay b1001Document988 pagesHrmsr83pay b1001Vinay KuchanaNo ratings yet