You might also like
- Leopold' ManeuversDocument3 pagesLeopold' Maneuversjava_biscocho122995% (22)
- Leopolds ManueverDocument5 pagesLeopolds ManueverRuby Dela RamaNo ratings yet
- Leopold ManeuverDocument4 pagesLeopold ManeuverElle100% (1)
- Essential Intrapartum and Newborn CareDocument3 pagesEssential Intrapartum and Newborn CareMasterclass40% (5)
- Nursing Care Plan Postpartum HemorrhageDocument2 pagesNursing Care Plan Postpartum Hemorrhagederic100% (60)
- Leopold's ManeuverDocument2 pagesLeopold's ManeuverDeanne Stephanie Hordista100% (4)
- Leopold's ManeuversDocument38 pagesLeopold's ManeuversGracy Morada Cu67% (6)
- Leopold's Maneuver PDFDocument13 pagesLeopold's Maneuver PDFBiway RegalaNo ratings yet
- Week 10.IMCI Case Study - BenDocument6 pagesWeek 10.IMCI Case Study - BenGeorgia Shayne CubeloNo ratings yet
- Einc ReviewerDocument4 pagesEinc ReviewerEricson Candelaria0% (1)
- Internal Examination: Prepared By: Lester D. Bongabong BSN Ii - BDocument9 pagesInternal Examination: Prepared By: Lester D. Bongabong BSN Ii - BJustine Cagatan100% (1)
- Final PPT - EincDocument75 pagesFinal PPT - EincJia Smith100% (3)
- Pedia 3.2 - IMCI (Vision) PDFDocument14 pagesPedia 3.2 - IMCI (Vision) PDFKaren ValdezNo ratings yet
- Ncm-107-Rle Evaluation ExamDocument11 pagesNcm-107-Rle Evaluation ExamMartin T ManuelNo ratings yet
- Immediate Newborn CareDocument3 pagesImmediate Newborn CareAlyssa Malsi NacinoNo ratings yet
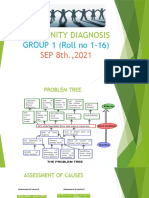
- COMMUNITY DIAGNOSIS Group 1Document11 pagesCOMMUNITY DIAGNOSIS Group 1Sumit GavitNo ratings yet
- Naegele's RuleDocument5 pagesNaegele's RuleSarah Jane MaganteNo ratings yet
- Percy JacksonDocument13 pagesPercy JacksonDawn Marco0% (2)
- Read Chapter 4 Minicase: Fondren Publishing, Inc. From The Sales Force Management Textbook by Mark W. Johnston & Greg W. MarshallDocument1 pageRead Chapter 4 Minicase: Fondren Publishing, Inc. From The Sales Force Management Textbook by Mark W. Johnston & Greg W. MarshallKJRNo ratings yet
- Leopold's ManeuverDocument2 pagesLeopold's ManeuverAnnaAlfonsoNo ratings yet
- Topic # 1 Leopold's ManueverDocument39 pagesTopic # 1 Leopold's ManueverJayrelle D. SafranNo ratings yet
- Leopold's ManeuverDocument22 pagesLeopold's ManeuverArlene Cerdeña Salceda100% (1)
- Essential Newborn Care: The DOH/WHO ProtocolDocument21 pagesEssential Newborn Care: The DOH/WHO ProtocolfelicitycherubNo ratings yet
- Leopold's ManeuverDocument2 pagesLeopold's ManeuverPJ AmolarNo ratings yet
- Nursing Care Management - 107: de La Salle Lipa College of NursingDocument3 pagesNursing Care Management - 107: de La Salle Lipa College of NursingThe Blue and Gold RvdNo ratings yet
- Unang YakapDocument3 pagesUnang YakapBernadeth Labrador100% (1)
- Infant Tub RationaleDocument4 pagesInfant Tub RationaleAllen Kenneth PacisNo ratings yet
- EINCDocument2 pagesEINCNess G. Mamasabulod100% (2)
- RLE Checklist Evaluation (Leopold's Maneuver)Document4 pagesRLE Checklist Evaluation (Leopold's Maneuver)Cameron De Guzman100% (1)
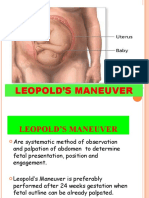
- Are Four Specific Steps in Palpating The Uterus Through The Abdomen in Order To Determine The Lie and Presentation of The FetusDocument2 pagesAre Four Specific Steps in Palpating The Uterus Through The Abdomen in Order To Determine The Lie and Presentation of The FetusMoiraMaeBeridoBalite100% (3)
- Concept of Unitive and Procreative HealthDocument5 pagesConcept of Unitive and Procreative HealthDONITA DALUMPINESNo ratings yet
- Assessment in PregnancyDocument15 pagesAssessment in PregnancyAna75% (4)
- Essential Intrapartum and Newborn CareDocument2 pagesEssential Intrapartum and Newborn CareKia potz100% (1)
- 4 Core Steps of Essential Newborn CareDocument2 pages4 Core Steps of Essential Newborn CareAl Ronald Vincent Marcelo81% (16)
- Leopolds Maneuvers Fundic Height Measurement and FHT Determination ChecklistDocument6 pagesLeopolds Maneuvers Fundic Height Measurement and FHT Determination ChecklistChristine Joy MolinaNo ratings yet
- Components of LaborDocument5 pagesComponents of LaborJeraldine Lindo100% (4)
- Labor and DeliveryDocument6 pagesLabor and DeliveryKenny NadelaNo ratings yet
- Essential Intrapartum and Newborn CareDocument23 pagesEssential Intrapartum and Newborn CareEarl ReyesNo ratings yet
- Leopolds Maneuver - Return DemoDocument1 pageLeopolds Maneuver - Return DemornrmmanphdNo ratings yet
- I. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsDocument5 pagesI. Framework For Maternal and Child Health Nursing (MCN) Focusing On At-Risk, High Risk, and Sick ClientsSophia Loraine Dorone Jesura100% (1)
- Problems of The PassengerDocument9 pagesProblems of The PassengerDanah Grace SanchezNo ratings yet
- CHN-Lecture Module 1 and 2Document64 pagesCHN-Lecture Module 1 and 2mirai desu100% (1)
- Procedure Guide Leopold's ManeuverDocument3 pagesProcedure Guide Leopold's ManeuverAubrey Justine GaleonNo ratings yet
- Po No Breast RationaleDocument4 pagesPo No Breast Rationalearnold john boniteNo ratings yet
- Typology of Nursing Problems in Family Health CareDocument7 pagesTypology of Nursing Problems in Family Health CareJunathan L. DelgadoNo ratings yet
- Signs of Placental SeparationDocument1 pageSigns of Placental SeparationMalou Yap Buot0% (1)
- MCN RLE Sitz Bath Procedure ChecklistDocument3 pagesMCN RLE Sitz Bath Procedure ChecklistHannah Angelu Cabading100% (1)
- Nursing Care of A Family Experiencing A Sudden Pregnancy: Flynne Chicay Butgui BSN 2BDocument92 pagesNursing Care of A Family Experiencing A Sudden Pregnancy: Flynne Chicay Butgui BSN 2BIra Delos SantosNo ratings yet
- Newborn Care ChecklistDocument5 pagesNewborn Care ChecklistAda Gay Olandia SerencioNo ratings yet
- Leopold's ManeuverDocument9 pagesLeopold's ManeuverAmiel Francisco Reyes100% (1)
- 10.theories of LaborDocument18 pages10.theories of LaborJulia Ramos100% (1)
- Rubric For Performing Fundal Height MeasurementDocument5 pagesRubric For Performing Fundal Height MeasurementPATRICIA JULIANNE CASTAÑETO RIVERANo ratings yet
- Table Presumptive Probable and Positive Signs of PregnancyDocument2 pagesTable Presumptive Probable and Positive Signs of Pregnancykylah gonzaga100% (1)
- Drug Study FormatDocument2 pagesDrug Study FormatDane CaumeranNo ratings yet
- Principles, Contents, and Steps: Clinical InstructorDocument25 pagesPrinciples, Contents, and Steps: Clinical InstructorWillie KitsNo ratings yet
- Home Visit and Bag TechniqueDocument34 pagesHome Visit and Bag TechniqueEdralyn MatalangNo ratings yet
- Leopold's Maneuver and 7 Cardinal MovementsDocument5 pagesLeopold's Maneuver and 7 Cardinal MovementsMikaela Gabrielle GERALINo ratings yet
- MCN Rle Lesson 5Document6 pagesMCN Rle Lesson 5Joeyca Shien PiolNo ratings yet
- Leopolds and FetalDocument7 pagesLeopolds and Fetaltyche100% (1)
- LEOPOLD's MANEUVER RATIONALEDocument3 pagesLEOPOLD's MANEUVER RATIONALEAngela AquisapNo ratings yet
- IntrapartumDocument16 pagesIntrapartumBrigitte CovarrubiasNo ratings yet
- Leopods ManeuverDocument8 pagesLeopods ManeuverDaryl Adrian RecaidoNo ratings yet
- Leopolds-Maneuver StudentsDocument40 pagesLeopolds-Maneuver StudentsCarlo GacadNo ratings yet
- IVT NotesDocument5 pagesIVT NotesChared LumbaNo ratings yet
- Postpartum Period HandoutsDocument8 pagesPostpartum Period HandoutsChared LumbaNo ratings yet
- Written Report: Lumba, Chared Joy D. BSN Ii-2 Group 7Document6 pagesWritten Report: Lumba, Chared Joy D. BSN Ii-2 Group 7Chared LumbaNo ratings yet
- DM FinaDocument3 pagesDM FinaChared LumbaNo ratings yet
- Submitted By: Lumba, Chared Joy D. BSN II-2/ Group 8 Submitted To: Ms. Sarah S. Nares, RN, MNDocument7 pagesSubmitted By: Lumba, Chared Joy D. BSN II-2/ Group 8 Submitted To: Ms. Sarah S. Nares, RN, MNChared LumbaNo ratings yet
- On Qbasic (Algorithm) : By: Nischit P.N. Pradhan Class: 10'B To: Prakash PradhanDocument6 pagesOn Qbasic (Algorithm) : By: Nischit P.N. Pradhan Class: 10'B To: Prakash Pradhanapi-364271112No ratings yet
- Philippines My Beloved (Rough Translation by Lara)Document4 pagesPhilippines My Beloved (Rough Translation by Lara)ARLENE FERNANDEZNo ratings yet
- Dwnload Full Conceptual Physics 12th Edition Hewitt Test Bank PDFDocument36 pagesDwnload Full Conceptual Physics 12th Edition Hewitt Test Bank PDFscreamsoaring.pm7hcv100% (13)
- Student Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415Document4 pagesStudent Health Services - 305 Estill Street Berea, KY 40403 - Phone: (859) 985-1415JohnNo ratings yet
- NIPMR Notification v3Document3 pagesNIPMR Notification v3maneeshaNo ratings yet
- Lesson Plan in Science III ObservationDocument2 pagesLesson Plan in Science III ObservationTrishaAnnSantiagoFidelNo ratings yet
- Masterlist of Private Elem. Schools S.Y. 2016 2017 Cavite ProvinceDocument17 pagesMasterlist of Private Elem. Schools S.Y. 2016 2017 Cavite ProvinceacinehhjNo ratings yet
- Presentation (AJ)Document28 pagesPresentation (AJ)ronaldNo ratings yet
- Datsasheet of LM347 IcDocument24 pagesDatsasheet of LM347 IcShubhamMittalNo ratings yet
- SiteVisit - Name (Done Excel, Pending CC)Document147 pagesSiteVisit - Name (Done Excel, Pending CC)CK AngNo ratings yet
- Chapter 2Document16 pagesChapter 2nannaNo ratings yet
- KFC 225 Installation ManualDocument2 pagesKFC 225 Installation Manualsunarya0% (1)
- Presentation On HR Department of Mobilink.Document18 pagesPresentation On HR Department of Mobilink.Sadaf YaqoobNo ratings yet
- Consumer Trend Canvas (CTC) Template 2022Document1 pageConsumer Trend Canvas (CTC) Template 2022Patricia DominguezNo ratings yet
- Timothy Ajani, "Syntax and People: How Amos Tutuola's English Was Shaped by His People"Document20 pagesTimothy Ajani, "Syntax and People: How Amos Tutuola's English Was Shaped by His People"PACNo ratings yet
- Tutorials in Complex Photonic Media SPIE Press Monograph Vol PM194 PDFDocument729 pagesTutorials in Complex Photonic Media SPIE Press Monograph Vol PM194 PDFBadunoniNo ratings yet
- An Improved Version of The Skin Chapter of Kent RepertoryDocument6 pagesAn Improved Version of The Skin Chapter of Kent RepertoryHomoeopathic PulseNo ratings yet
- The Distracted Mind - ExcerptDocument15 pagesThe Distracted Mind - Excerptwamu885No ratings yet
- Edir AdminDocument916 pagesEdir AdminSELIMNo ratings yet
- Activity 2Document2 pagesActivity 2cesar jimenezNo ratings yet
- MarketingDocument5 pagesMarketingRose MarieNo ratings yet
- Taxation and LibertyDocument28 pagesTaxation and LibertyRitu Raj RamanNo ratings yet
- Performance Task in Mathematics 10 First Quarter: GuidelinesDocument2 pagesPerformance Task in Mathematics 10 First Quarter: Guidelinesbelle cutiee100% (3)
- TesisDocument388 pagesTesisHadazaNo ratings yet
- Fundamentals of Marketing Management: by Prabhat Ranjan Choudhury, Sr. Lecturer, B.J.B (A) College, BhubaneswarDocument53 pagesFundamentals of Marketing Management: by Prabhat Ranjan Choudhury, Sr. Lecturer, B.J.B (A) College, Bhubaneswarprabhatrc4235No ratings yet
- Course Hand Out Comm. Skill BSC AgDocument2 pagesCourse Hand Out Comm. Skill BSC Agfarid khanNo ratings yet
- Securities and Exchange Commission: Non-Holding of Annual MeetingDocument2 pagesSecurities and Exchange Commission: Non-Holding of Annual MeetingBea AlonzoNo ratings yet
- The First Step Analysis: 1 Some Important DefinitionsDocument4 pagesThe First Step Analysis: 1 Some Important DefinitionsAdriana Neumann de OliveiraNo ratings yet