You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- TADs in Orthodontics: Miniplates for Class III CorrectionDocument18 pagesTADs in Orthodontics: Miniplates for Class III CorrectionimtiyazorthodontistNo ratings yet
- Total Arch Distalization A ReviewDocument4 pagesTotal Arch Distalization A ReviewsmritiNo ratings yet
- Classification of Failure of FPDDocument4 pagesClassification of Failure of FPDrayavarapu sunilNo ratings yet
- Development of Teeth 1Document37 pagesDevelopment of Teeth 1Muli MaroshiNo ratings yet
- Herbst ApplianceDocument21 pagesHerbst Applianceimtiyazorthodontist83% (6)
- A Review of Attachments For Removable Partial Denture Design Part 2 90Document7 pagesA Review of Attachments For Removable Partial Denture Design Part 2 90alioossaNo ratings yet
- Pulp Therapy in ChildrenDocument4 pagesPulp Therapy in ChildrenshahinshamshiriNo ratings yet
- Applications of Orthodontic Mini-ImplantsDocument277 pagesApplications of Orthodontic Mini-ImplantsNicolas Homsi100% (1)
- Are Occulsion and Comprehensive Dentistry Really That ImportantDocument20 pagesAre Occulsion and Comprehensive Dentistry Really That ImportantAhmed HamzaNo ratings yet
- OrthodonticsDocument14 pagesOrthodonticsimtiyazorthodontistNo ratings yet
- Cephalometrics Manual KrothDocument124 pagesCephalometrics Manual Krothimtiyazorthodontist100% (3)
- Ceph Analysis LabDocument23 pagesCeph Analysis LabimtiyazorthodontistNo ratings yet
- KimDocument12 pagesKimIvanna H. A.No ratings yet
- K9 Ve Balista Spring Başarı OranlarıDocument8 pagesK9 Ve Balista Spring Başarı OranlarıRümeysa AydınNo ratings yet
- Occlusal Indices GuideDocument229 pagesOcclusal Indices GuideRajshekhar BanerjeeNo ratings yet
- 1Document11 pages1Gowri KannanNo ratings yet
- Basic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationDocument4 pagesBasic Principles of Obturator Design For Partially Edentulous Patients. Part I: ClassificationArun PrasadNo ratings yet
- Arch Expansion DR SaadDocument41 pagesArch Expansion DR Saadahmed saad100% (1)
- Orthodontist's Perceptions of Smile EstheticsA Questionnaire Based StudyDocument5 pagesOrthodontist's Perceptions of Smile EstheticsA Questionnaire Based StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Biomechanics of the Edentulous StateDocument30 pagesBiomechanics of the Edentulous StateAishwarya SharmaNo ratings yet
- Interrelationship Between Periodontics and Restorative DentistryDocument19 pagesInterrelationship Between Periodontics and Restorative DentistrySuperna TiwariNo ratings yet
- New Clasp Assembly For Distal Extension Removable Partial DenturesDocument17 pagesNew Clasp Assembly For Distal Extension Removable Partial DenturesAli FaridiNo ratings yet
- Biological Considerations in Operative DentistryDocument8 pagesBiological Considerations in Operative Dentistrysheryl teoNo ratings yet
- Jurnal Ilmu Konservasi Gigi: PSA Pada Supernumery RootDocument6 pagesJurnal Ilmu Konservasi Gigi: PSA Pada Supernumery RootAchmad Zam Zam AghazyNo ratings yet
- Historia Diente Ro 01-Cecilia-BacaliDocument5 pagesHistoria Diente Ro 01-Cecilia-BacaliAARON DIAZ RONQUILLONo ratings yet
- PDF PreviewDocument5 pagesPDF PreviewCatalin MNo ratings yet
- Digitally Enhanced Esthetic DentistryDocument3 pagesDigitally Enhanced Esthetic DentistrySMART SMARNo ratings yet
- Maxillary Permanent Central IncisorsDocument68 pagesMaxillary Permanent Central IncisorsAmit Singh100% (1)
- Placa de Acetato BioartDocument5 pagesPlaca de Acetato BioartlenzajrNo ratings yet
- Essential Lines DR ChioderaDocument7 pagesEssential Lines DR ChioderaajiargoputroNo ratings yet
- Periodontal Diseases in Children PedoDocument34 pagesPeriodontal Diseases in Children Pedoarpita7dr9693No ratings yet
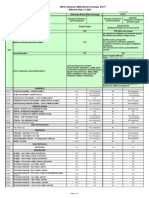
- MCS Classicare (MA) Dental Coverage SummaryDocument4 pagesMCS Classicare (MA) Dental Coverage SummaryJessicaNo ratings yet
- Custom Post and Core Case ReportDocument10 pagesCustom Post and Core Case ReportDrAditya BansalNo ratings yet
- Spark Erosion Step by Step GuideDocument4 pagesSpark Erosion Step by Step GuideDentist HereNo ratings yet
- 01 - Introduction To DentistryDocument18 pages01 - Introduction To Dentistrymichal ben meronNo ratings yet
- Intraoral Radiographic Techniques ǁ: by Dr. WajnaaDocument32 pagesIntraoral Radiographic Techniques ǁ: by Dr. WajnaaALI abd-alamamNo ratings yet
- Periodontal Mechanoreceptors Stimulated Study of Human Masseter ReflexDocument6 pagesPeriodontal Mechanoreceptors Stimulated Study of Human Masseter ReflexRakesh KumarNo ratings yet