You might also like
- HPS Endoscope Decontamination 2004 PDFDocument190 pagesHPS Endoscope Decontamination 2004 PDFHong-Nam Kim100% (1)
- Esgena CDC Endos PDFDocument30 pagesEsgena CDC Endos PDFErfandi ZeinNo ratings yet
- Endoscope DisinfectionDocument14 pagesEndoscope Disinfectioneliasox123No ratings yet
- Position Statement: Reco Mme Ndati O NsDocument9 pagesPosition Statement: Reco Mme Ndati O NsAhana MukherjeeNo ratings yet
- FUSIC Decontamination GuidelinesDocument2 pagesFUSIC Decontamination GuidelinesMarcelo UGNo ratings yet
- ENT UK Guidelines - Decontamination of Flexible and Rigid Endoscopes 2017Document14 pagesENT UK Guidelines - Decontamination of Flexible and Rigid Endoscopes 2017Luis De jesus SolanoNo ratings yet
- Shpa Standards of Practice For The Safe Handling of Cytotoxic DR 2005Document9 pagesShpa Standards of Practice For The Safe Handling of Cytotoxic DR 2005Lan FdzNo ratings yet
- 2013 - BestPractices For HLDDocument53 pages2013 - BestPractices For HLDDaniela Cirnatu100% (1)
- Vitalograph - Hygiene Considerations For SpirometryDocument4 pagesVitalograph - Hygiene Considerations For SpirometryEileenYingYeeNo ratings yet
- Fresenius+Dialysis+Machine+Disinfection V1 0Document7 pagesFresenius+Dialysis+Machine+Disinfection V1 0Mendes NovatoNo ratings yet
- SiD 4.3.3.3 at 7 June 2011Document4 pagesSiD 4.3.3.3 at 7 June 2011Dr-Mohamed KandeelNo ratings yet
- Endoscope Reprocessing Risk and Current Risk PracticeDocument65 pagesEndoscope Reprocessing Risk and Current Risk PracticeHosam GomaaNo ratings yet
- Transporting Soiled InstrumentsDocument3 pagesTransporting Soiled InstrumentsRAZNAS ASLAM A KNo ratings yet
- Delays in Endoscope Reprocessing and The Biofilms WithinDocument12 pagesDelays in Endoscope Reprocessing and The Biofilms WithinHAITHM MURSHEDNo ratings yet
- Prep For Joint Commissions RV yDocument12 pagesPrep For Joint Commissions RV yKevin Adam RobinsterNo ratings yet
- 6 Reprocessing of EndosDocument28 pages6 Reprocessing of Endoshananshosha743No ratings yet
- Reprocessing of Flexible Cystoscopes: Joint AUA/SUNA White Paper On TheDocument15 pagesReprocessing of Flexible Cystoscopes: Joint AUA/SUNA White Paper On Theأحمد العريقيNo ratings yet
- Endoscope ReprocessingDocument34 pagesEndoscope Reprocessingmonir61100% (1)
- Multisociety Guideline Reprocessing Gi EndoscopesDocument29 pagesMultisociety Guideline Reprocessing Gi EndoscopesVivy Ortega MoreiraNo ratings yet
- Dissertação Traduzida-Juliana. (1)Document19 pagesDissertação Traduzida-Juliana. (1)Alessandro Sousa NascimentoNo ratings yet
- Case Scenario Evidence Base PracticeDocument4 pagesCase Scenario Evidence Base Practicemaria khalifaNo ratings yet
- Clinical Nutrition Experimental: MethodologyDocument6 pagesClinical Nutrition Experimental: MethodologyMariana BustamanteNo ratings yet
- Flexible Endoscope Reprocessors, Automatic PDFDocument31 pagesFlexible Endoscope Reprocessors, Automatic PDFJonathan DuranNo ratings yet
- 2012 PROF 174 Ophthalmic Instrument Decontamination PDFDocument18 pages2012 PROF 174 Ophthalmic Instrument Decontamination PDFmochkurniawanNo ratings yet
- ANESTESIDocument13 pagesANESTESIChachaNo ratings yet
- Guidelines For The Cleaning and Sterilization Of.14Document9 pagesGuidelines For The Cleaning and Sterilization Of.14Ana Mª GuaiquilNo ratings yet
- ESH-IP 2010 Protocol PDFDocument16 pagesESH-IP 2010 Protocol PDFias2008No ratings yet
- Infections Associated With Reprocessed Urological Endoscopes - Letter To Health Care Providers - FDADocument3 pagesInfections Associated With Reprocessed Urological Endoscopes - Letter To Health Care Providers - FDAt merchant100% (1)
- Guidelines For Safety in The Gastrointestinal Endoscopy UnitDocument10 pagesGuidelines For Safety in The Gastrointestinal Endoscopy UnitDairotul KhasanahNo ratings yet
- Guidelines On Cleaning and Disinfection in GI Endoscopy: E.S.G.E. GuidelinesDocument7 pagesGuidelines On Cleaning and Disinfection in GI Endoscopy: E.S.G.E. GuidelinesSailu KatragaddaNo ratings yet
- Quality Assurance and Tracing of Endoscope ReprocessingDocument26 pagesQuality Assurance and Tracing of Endoscope ReprocessingHosam Gomaa100% (1)
- Best Practices in PhlebotomyDocument8 pagesBest Practices in PhlebotomyPrincess WeiyoungNo ratings yet
- Tonometer Sterilisation SurveyDocument4 pagesTonometer Sterilisation SurveyPhilip McNelsonNo ratings yet
- Tugas Kelompok 2 BHS Inggris SopDocument17 pagesTugas Kelompok 2 BHS Inggris Sopmoms naraNo ratings yet
- Comparison of Air Samplers For Environmental Monitoring Regarding ISO 14698Document8 pagesComparison of Air Samplers For Environmental Monitoring Regarding ISO 14698singam5383727No ratings yet
- Guideline For Ultrasound Transducer Cleaning and DisinfectionDocument4 pagesGuideline For Ultrasound Transducer Cleaning and DisinfectiondocbinNo ratings yet
- Pidsr Manual On Infection ControlDocument4 pagesPidsr Manual On Infection ControlKristine EstrellaNo ratings yet
- Articlealdehydes Hyg Med 2006 Van DrongelenDocument5 pagesArticlealdehydes Hyg Med 2006 Van DrongelenOMAR EL HAMDAOUINo ratings yet
- Guidelines For The Cleaning and Sterilization Of.1Document2 pagesGuidelines For The Cleaning and Sterilization Of.1Ana Mª GuaiquilNo ratings yet
- Guidline of Management of Porta CathDocument8 pagesGuidline of Management of Porta CathroncekeyNo ratings yet
- Ensuring Safety of Endoscopic ProceduresDocument3 pagesEnsuring Safety of Endoscopic Proceduresmonir61No ratings yet
- Immediate Post-Anaesthesia Recovery 2013Document20 pagesImmediate Post-Anaesthesia Recovery 2013gythrieNo ratings yet
- Isolation and Enumeration of Aeromonas and Pseudomonas aeruginosaDocument40 pagesIsolation and Enumeration of Aeromonas and Pseudomonas aeruginosaDavid WoodsNo ratings yet
- pp45 47 CSJJun19Document3 pagespp45 47 CSJJun19Андрій КасійNo ratings yet
- MED. Dental Services (Infectionn Control 1) .003docDocument7 pagesMED. Dental Services (Infectionn Control 1) .003docKenny JosefNo ratings yet
- 2014 - Guidelines For Safety in The Gastrointestinal Endoscopy Unit PDFDocument10 pages2014 - Guidelines For Safety in The Gastrointestinal Endoscopy Unit PDFBaim FarmaNo ratings yet
- 9 enDocument15 pages9 enDestiny TobiNo ratings yet
- ReprocessingendoscopesDocument10 pagesReprocessingendoscopesClara MedinaNo ratings yet
- Best Practices in PhlebotomyDocument125 pagesBest Practices in PhlebotomyShiki Asagami BrunestedNo ratings yet
- AARC Clinical Practice Guidelines - Artificial Airway SuctioningDocument14 pagesAARC Clinical Practice Guidelines - Artificial Airway Suctioningaperfectcircle7978No ratings yet
- PNP 034831Document9 pagesPNP 034831Celso BelalaNo ratings yet
- ISOPP Safe Handling of Cytotoxics (024-034)Document11 pagesISOPP Safe Handling of Cytotoxics (024-034)Yuli AmaliaNo ratings yet
- DOwnoad 1Document7 pagesDOwnoad 1Ahmad ZaidiNo ratings yet
- WP Medical Device Endotoxin TestingDocument6 pagesWP Medical Device Endotoxin TestingJeevanend ArumugamNo ratings yet
- Aorn 12784Document10 pagesAorn 12784Yahia HassaanNo ratings yet
- Regulations for autoclave use at UCDocument8 pagesRegulations for autoclave use at UCJoão Paulo LoboNo ratings yet
- 260 Ijar-8550 3Document13 pages260 Ijar-8550 3esraa asemNo ratings yet
- Sensors 23 03710Document21 pagesSensors 23 03710hani1986yeNo ratings yet
- Sensors 23 03684 v2Document12 pagesSensors 23 03684 v2hani1986yeNo ratings yet
- Sensors 23 03723Document18 pagesSensors 23 03723hani1986yeNo ratings yet
- Brainsci 13 00593Document11 pagesBrainsci 13 00593hani1986yeNo ratings yet
- Brainsci 13 00598Document16 pagesBrainsci 13 00598hani1986yeNo ratings yet
- Sensors 23 03714Document22 pagesSensors 23 03714hani1986yeNo ratings yet
- Sensors 23 03718Document21 pagesSensors 23 03718hani1986yeNo ratings yet
- Brainsci 13 00597Document12 pagesBrainsci 13 00597hani1986yeNo ratings yet
- Comparative Analysis of Various Filtering Techniques For Denoising EEG SignalsDocument4 pagesComparative Analysis of Various Filtering Techniques For Denoising EEG Signalshani1986yeNo ratings yet
- Brainsci 13 00614Document11 pagesBrainsci 13 00614hani1986yeNo ratings yet
- Decoding of Pain Perception Using EEG Signals For A Real-Time Reflex System in Prostheses: A Case StudyDocument11 pagesDecoding of Pain Perception Using EEG Signals For A Real-Time Reflex System in Prostheses: A Case Studyhani1986yeNo ratings yet
- Brainsci 13 00612Document18 pagesBrainsci 13 00612hani1986yeNo ratings yet
- Brainsci 13 00609Document17 pagesBrainsci 13 00609hani1986yeNo ratings yet
- Brainsci 13 00589 v2Document22 pagesBrainsci 13 00589 v2hani1986yeNo ratings yet
- Battery Back Up User ManualDocument2 pagesBattery Back Up User Manualhani1986yeNo ratings yet
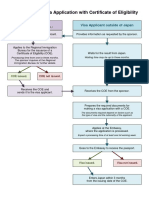
- Flow Chart For Visa Application With Certificate of EligibilityDocument1 pageFlow Chart For Visa Application With Certificate of EligibilitySyed Sufyian AliNo ratings yet
- Chemistry InstrumentsDocument19 pagesChemistry Instrumentshani1986yeNo ratings yet
- دورة في الماتلاب MATLABDocument60 pagesدورة في الماتلاب MATLABأكبر مكتبة كتب عربية33% (3)
- Salatpanel Usermanual Int V50above INT PDFDocument12 pagesSalatpanel Usermanual Int V50above INT PDFhani1986yeNo ratings yet
- Review and Analysis of The Egyptian Tender Law and Its Executive RegulationsDocument22 pagesReview and Analysis of The Egyptian Tender Law and Its Executive Regulationshani1986ye100% (1)
- The Silicon Laboratories C8051F020Document89 pagesThe Silicon Laboratories C8051F020hani1986yeNo ratings yet
- Database Management:: Ray R. Larson University of California, Berkeley School of Information Management and SystemsDocument51 pagesDatabase Management:: Ray R. Larson University of California, Berkeley School of Information Management and Systemshani1986yeNo ratings yet
- Funnel VolumesDocument6 pagesFunnel Volumeshani1986yeNo ratings yet
- Flow Chart For Visa Application With Certificate of EligibilityDocument1 pageFlow Chart For Visa Application With Certificate of EligibilitySyed Sufyian AliNo ratings yet
- Using Excel 2010 With Statistics For Managers Using Microsoft Excel 6th Edition PDFDocument3 pagesUsing Excel 2010 With Statistics For Managers Using Microsoft Excel 6th Edition PDFhani1986yeNo ratings yet
- Logiqp5 TransducersDocument4 pagesLogiqp5 Transducershani1986yeNo ratings yet
- Design of FIR LS Hibert Transformers Through Fuliband TorsDocument5 pagesDesign of FIR LS Hibert Transformers Through Fuliband Torshani1986yeNo ratings yet
- Trbl-Ar287 337 407 507Document10 pagesTrbl-Ar287 337 407 507hani1986yeNo ratings yet
- An Introduction To Marketing NutritionDocument22 pagesAn Introduction To Marketing NutritionlfamaroNo ratings yet
- Current IssuesDocument20 pagesCurrent IssuesPat MillerNo ratings yet
- Test Bank For Nutrition Essentials For Nursing Practice 8th North American Edition Susan G DudekDocument19 pagesTest Bank For Nutrition Essentials For Nursing Practice 8th North American Edition Susan G Dudekluongbellamylkg100% (22)
- Gummy Bear - Nadhirah PDFDocument38 pagesGummy Bear - Nadhirah PDFNadhirah Hamzah0% (1)
- Adenoviruses and Other Common VirusesDocument95 pagesAdenoviruses and Other Common VirusesSaima ZuberiNo ratings yet
- Top 10 Environmental DisastersDocument26 pagesTop 10 Environmental Disastersifa_saimiNo ratings yet
- BSG Guidelines Decontamination of Equipment For Gastrointestinal EndosDocument25 pagesBSG Guidelines Decontamination of Equipment For Gastrointestinal Endoshani1986yeNo ratings yet
- Biochemical and Biophysical Research CommunicationsDocument5 pagesBiochemical and Biophysical Research CommunicationsAlejandra Gomez RuizNo ratings yet
- Manual AphisDocument967 pagesManual AphisVera Valenzuela HinojosaNo ratings yet
- Animals: Euthanasia of Cattle: Practical Considerations and ApplicationDocument17 pagesAnimals: Euthanasia of Cattle: Practical Considerations and ApplicationBlueyNo ratings yet
- IPO 2022 SRO No. 545I 2022 Dt. 22.4 2022Document240 pagesIPO 2022 SRO No. 545I 2022 Dt. 22.4 2022Faizullah MagsiNo ratings yet
- Livestock Mortality Composting For Large and Small Operations in The Semi-Arid WestDocument28 pagesLivestock Mortality Composting For Large and Small Operations in The Semi-Arid WestslupisNo ratings yet
- Creutzfeldt JakobDocument6 pagesCreutzfeldt JakobErnesto Ochoa MonroyNo ratings yet
- 10 IM Food MicroDocument23 pages10 IM Food MicroNader SedighiNo ratings yet
- Cleaning Product SDSDocument4 pagesCleaning Product SDSSyaiful AnwarNo ratings yet
- 217 CTI-SCSC FoodSafety FN PDFDocument20 pages217 CTI-SCSC FoodSafety FN PDFMinh PhamNo ratings yet
- Ielts General Training Volume 6 Listening Practice Test 2 v9 61248Document28 pagesIelts General Training Volume 6 Listening Practice Test 2 v9 61248Artur BochkivskiyNo ratings yet
- Indian Meat Industry: Opportunities and Challenges: January 2011Document7 pagesIndian Meat Industry: Opportunities and Challenges: January 2011satyajitNo ratings yet
- Veggie Works Vegan CookbookDocument777 pagesVeggie Works Vegan Cookbookx01x100% (2)
- Don't Worry (It's Safe To Eat) - The True Story of GM Food, BSE and Foot and MouthDocument281 pagesDon't Worry (It's Safe To Eat) - The True Story of GM Food, BSE and Foot and Mouthnaconi011100% (1)
- Globalization Threatens French Cultural IdentityDocument10 pagesGlobalization Threatens French Cultural IdentityOkebs Young BossNo ratings yet
- Lab Medical International Vol.28.6-7Document68 pagesLab Medical International Vol.28.6-7Iguodala OwieNo ratings yet
- Meat ScienceDocument320 pagesMeat ScienceVivian Feddern100% (3)
- Ups Export ManualDocument25 pagesUps Export Manuals.srinivas36No ratings yet
- Gourmet MeatsDocument34 pagesGourmet MeatsAmi BennounaNo ratings yet
- General Absence DeclarationDocument5 pagesGeneral Absence DeclarationAparesh GantaitNo ratings yet
- Rethinkingthe Regiulations For Food WasteDocument10 pagesRethinkingthe Regiulations For Food WasteglomepapiNo ratings yet
- Buffalo Meat Imports and The Philippine Livestock Industry-An Impact AssessmentDocument20 pagesBuffalo Meat Imports and The Philippine Livestock Industry-An Impact AssessmentKatrina Santos100% (1)
- Registration Requirments of Animal Derived Non Medicated ProductsDocument2 pagesRegistration Requirments of Animal Derived Non Medicated ProductsValeria DumitrescuNo ratings yet
- CIS-GCC Countries Brief and Existing Trade of PakistanDocument85 pagesCIS-GCC Countries Brief and Existing Trade of PakistanMehdiNo ratings yet