You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- South Africa CMV Viral Load Testing May2015Document4 pagesSouth Africa CMV Viral Load Testing May2015EnergadeNo ratings yet
- The Social Impact of Covid-19Document1 pageThe Social Impact of Covid-19Trisha MaguikayNo ratings yet
- Genetics - PYQs and Concept Maps-AKDocument92 pagesGenetics - PYQs and Concept Maps-AKSaiNagaVignesh BandhamNo ratings yet
- Preoperative Hair Removal A Case Report With Implications ForDocument32 pagesPreoperative Hair Removal A Case Report With Implications ForJasmine RogersNo ratings yet
- QPCM, Specimen Collection Guide, Mount Sinai, GovDocument74 pagesQPCM, Specimen Collection Guide, Mount Sinai, GovFilipus HendiantoNo ratings yet
- Department of Genetics: Covid-19 RT PCRDocument1 pageDepartment of Genetics: Covid-19 RT PCRSahil AnsariNo ratings yet
- November 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Document20 pagesNovember 9, 2011 Emily Gogarty Chris Sokoloff Queen's University MECH478Chris SoksNo ratings yet
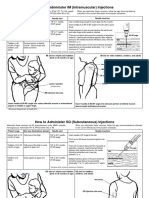
- Im SQ Admin PDFDocument2 pagesIm SQ Admin PDFAlvin JjNo ratings yet
- Laboratory Test Report: Test Name Result Sars-Cov-2Document1 pageLaboratory Test Report: Test Name Result Sars-Cov-2Karthikeya MoorthyNo ratings yet
- Neonatology Cambridge Pocket ClinicianDocument601 pagesNeonatology Cambridge Pocket Clinicianjuanse1994No ratings yet
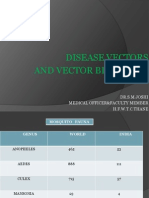
- Disease Vectors and Vector BionomicsDocument16 pagesDisease Vectors and Vector BionomicsSuhas JoshiNo ratings yet
- MedChem10 Antiviral PDFDocument85 pagesMedChem10 Antiviral PDFMартин ДончевNo ratings yet
- Viral Meningitis: David R. ChadwickDocument14 pagesViral Meningitis: David R. ChadwickVina HardiantiNo ratings yet
- GA Mongolia Position PaperDocument3 pagesGA Mongolia Position PaperSri RezekiNo ratings yet
- A Case Study of Ankylosing SpondylitisDocument10 pagesA Case Study of Ankylosing SpondylitisVenkatesan VidhyaNo ratings yet
- Salivary GlandsDocument68 pagesSalivary GlandsTatiana Decuseară100% (1)
- A. Definition: Septic ShockDocument9 pagesA. Definition: Septic ShockKimberly Subade MandilagNo ratings yet
- Retro VirDocument3 pagesRetro VirJericho MangalinNo ratings yet
- Specific Nursing Care Rendered in Hepatic Encephalopathy Contemporary Review and New Clinical Insights 2167 1168 1000264Document7 pagesSpecific Nursing Care Rendered in Hepatic Encephalopathy Contemporary Review and New Clinical Insights 2167 1168 1000264zeljko_vlaisavl4859No ratings yet
- Mycobacterium smegmatis Research OverviewDocument6 pagesMycobacterium smegmatis Research OverviewSalil ShauNo ratings yet
- Chronic Rhinitis Types and CausesDocument14 pagesChronic Rhinitis Types and CausesGunawan AliNo ratings yet
- Hiv Current Trend in The Use of HaartDocument19 pagesHiv Current Trend in The Use of Haartapi-3705046No ratings yet
- E. faecalis Endodontic ChallengeDocument5 pagesE. faecalis Endodontic ChallengeMonica RoopChanderNo ratings yet
- Toacs 2Document215 pagesToacs 2Mobin Ur Rehman Khan100% (1)
- Best Practices To Control Late BlightDocument34 pagesBest Practices To Control Late BlightJorge Luis Alonso G.No ratings yet
- Septic Shock Nursing Assessment and ManagementDocument6 pagesSeptic Shock Nursing Assessment and ManagementJenn GallowayNo ratings yet
- Osce SuturingDocument3 pagesOsce Suturingdaniel ragonjanNo ratings yet
- Igas Flow ChartDocument1 pageIgas Flow ChartYi Wei KoNo ratings yet
- Hidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkDocument52 pagesHidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkEira LopezNo ratings yet
- Maths Coursework JDocument5 pagesMaths Coursework JAnimaNo ratings yet