You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Constitution and By-Laws of The New Jersey Republican State CommitteeDocument6 pagesConstitution and By-Laws of The New Jersey Republican State CommitteeNJGOPNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- LEGAL OPINION-wetland 2020Document3 pagesLEGAL OPINION-wetland 2020Athena SalasNo ratings yet
- Memorial RespondentDocument23 pagesMemorial RespondentDevender Yadav100% (1)
- MUN Resolution - Cyber SecurityDocument3 pagesMUN Resolution - Cyber SecurityMinh Vu0% (1)
- Down Cobbled Streets, Phil O'Keefe Pp.22-31Document7 pagesDown Cobbled Streets, Phil O'Keefe Pp.22-31niiamhbrennanNo ratings yet
- Good News About Irish ResearchDocument42 pagesGood News About Irish ResearchniiamhbrennanNo ratings yet
- Housing (Miscellaneous Provisions) Act, 1931Document43 pagesHousing (Miscellaneous Provisions) Act, 1931niiamhbrennanNo ratings yet
- Dail Eireann - Vol 61-23 April1936Document51 pagesDail Eireann - Vol 61-23 April1936niiamhbrennanNo ratings yet
- Maguire, Joseph, The Housing Problem in Ireland and Great Britain and The Essentials of Its SolutionDocument14 pagesMaguire, Joseph, The Housing Problem in Ireland and Great Britain and The Essentials of Its Solutionniiamhbrennan100% (2)
- Canavan, J.E., Slum Clearance in DublinDocument12 pagesCanavan, J.E., Slum Clearance in DublinniiamhbrennanNo ratings yet
- Irish Tuberculosis Death Rates - Counihan, J.E. & Dillon, T.W.T. 1944Document20 pagesIrish Tuberculosis Death Rates - Counihan, J.E. & Dillon, T.W.T. 1944niiamhbrennanNo ratings yet
- (TARA) Tuberculosis Mortality Rates - Geary, R.C. 1930Document37 pages(TARA) Tuberculosis Mortality Rates - Geary, R.C. 1930niiamhbrennanNo ratings yet
- Unskilled Labour in DublinDocument16 pagesUnskilled Labour in DublinniiamhbrennanNo ratings yet
- Trump V VanceDocument68 pagesTrump V VanceStefan Becket67% (3)
- TAKING RIGHTS SERIOUSLY. by Ronald Dworkin. Massachusetts - HarvarDocument18 pagesTAKING RIGHTS SERIOUSLY. by Ronald Dworkin. Massachusetts - HarvarEvolbooksNo ratings yet
- PIL CasesDocument297 pagesPIL CasesAleah-Hidaya Ali Hadji RakhimNo ratings yet
- State Personnel Board Resolution and Order Following Investigative Hearing Case 13-1216ADocument20 pagesState Personnel Board Resolution and Order Following Investigative Hearing Case 13-1216AJon Ortiz100% (1)
- Timoner V PeopleDocument6 pagesTimoner V PeopleKanraMendozaNo ratings yet
- Roadway Obstruction Amendments: Be It Enacted by The Legislature of The State of UtahDocument2 pagesRoadway Obstruction Amendments: Be It Enacted by The Legislature of The State of UtahAlyssa RobertsNo ratings yet
- Its Importance: MarketingDocument20 pagesIts Importance: MarketingAbdullah JavedNo ratings yet
- CSDG Papers: State Responsiveness To Public Security Needs: The Politics of Security Decision-MakingDocument56 pagesCSDG Papers: State Responsiveness To Public Security Needs: The Politics of Security Decision-Makingkipperfletcher23No ratings yet
- Res Judicata and Lis Pendens in Investment ArbitrationDocument16 pagesRes Judicata and Lis Pendens in Investment Arbitrationrachel malingkasNo ratings yet
- Dev Dutt v. Union of IndiaDocument9 pagesDev Dutt v. Union of IndiaMayankNo ratings yet
- Social Media Marketing ProposalDocument4 pagesSocial Media Marketing Proposalpriyanka goelNo ratings yet
- Casemine Judgment 89996Document3 pagesCasemine Judgment 89996Imbisaat LiyaqatNo ratings yet
- Distribution of Legislative Powers WRT Doctrine of Pith and SubstanceDocument37 pagesDistribution of Legislative Powers WRT Doctrine of Pith and SubstanceSaravna Vasanta100% (1)
- Public Safety Officers Advance Course: Student Individual Program PlanDocument10 pagesPublic Safety Officers Advance Course: Student Individual Program PlanMaria Fiona Duran Merquita100% (2)
- Combinepdf PDFDocument399 pagesCombinepdf PDFPuppyNo ratings yet
- Baltazar V People, G R No 174016, July 28, 2008, 582 PHIL 275 294Document12 pagesBaltazar V People, G R No 174016, July 28, 2008, 582 PHIL 275 294Jett ChuaquicoNo ratings yet
- Integrated Marketing Communication Plan Powerpoint PPT Template BundlesDocument21 pagesIntegrated Marketing Communication Plan Powerpoint PPT Template BundlesShyna GargNo ratings yet
- Criminal Procedure Riano NotesDocument55 pagesCriminal Procedure Riano NotesAKnownKneeMouseeNo ratings yet
- Food Safety and Standards (Salary, Allowances and Other Conditions of Services of Officers and Employees) Regulations 2013Document12 pagesFood Safety and Standards (Salary, Allowances and Other Conditions of Services of Officers and Employees) Regulations 2013Latest Laws TeamNo ratings yet
- Chapter X CRPCDocument10 pagesChapter X CRPCAkshay SarjanNo ratings yet
- University of Botswana: InstructionsDocument5 pagesUniversity of Botswana: InstructionsTess JackNo ratings yet
- The British Judiciary: Unit 4Document76 pagesThe British Judiciary: Unit 4anemajaNo ratings yet
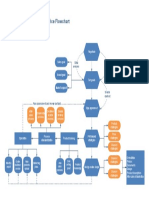
- Ecommerce FlowchartDocument1 pageEcommerce FlowchartkarmayagnaNo ratings yet
- CD Bersabal v. SalvadorDocument4 pagesCD Bersabal v. Salvador123014stephenNo ratings yet
- Fresher' Moot - FM24 - Memorial For The Respondent 1Document24 pagesFresher' Moot - FM24 - Memorial For The Respondent 1dildharNo ratings yet
- Court Notes From Daniel Norment's July 6 Zoom HearingDocument1 pageCourt Notes From Daniel Norment's July 6 Zoom HearingLenny CohenNo ratings yet