You might also like
- Renal Diet Plan & Cookbook: The Optimal Nutrition Guide to Manage Kidney DiseaseFrom EverandRenal Diet Plan & Cookbook: The Optimal Nutrition Guide to Manage Kidney DiseaseNo ratings yet
- Liver CirrhosisDocument31 pagesLiver CirrhosisAsniah Hadjiadatu Abdullah100% (1)
- CP - Liver CirrhosisDocument161 pagesCP - Liver CirrhosisRomeo ReyesNo ratings yet
- Case Liver CirrhosisDocument73 pagesCase Liver CirrhosisJesus Orita-Delima100% (1)
- Chronic Renal FailureDocument28 pagesChronic Renal FailurePatricia Nadine Sarcadio NeffeNo ratings yet
- Case Study Liver CirrhosisDocument30 pagesCase Study Liver CirrhosisMarielle Soriano100% (3)
- Liver Cirrhosis Case PresentationDocument146 pagesLiver Cirrhosis Case Presentationjennachristy0395% (21)
- Liver Cirrhosis: A Case Study OnDocument31 pagesLiver Cirrhosis: A Case Study OnCharmaine del RosarioNo ratings yet
- My Case Study of Liver CirrhosisDocument13 pagesMy Case Study of Liver Cirrhosisdysphile100% (1)
- Case Study - Acute PancreatitisDocument12 pagesCase Study - Acute Pancreatitisfoe_azishan_kazaff100% (2)
- Case Study On Cirrhosis of LiverDocument21 pagesCase Study On Cirrhosis of LiverAlpit Gandhi67% (3)
- Liver CirrhosisDocument76 pagesLiver Cirrhosiskathy100% (2)
- Case Study On Alcoholic Liver DiseaseDocument24 pagesCase Study On Alcoholic Liver DiseaseKristine Alejandro100% (5)
- Case Study-Congestive Heart FailureDocument71 pagesCase Study-Congestive Heart FailureKentTangcalagan92% (13)
- CHF Case StudyDocument38 pagesCHF Case StudyMelissa David100% (1)
- Case Study Liver CirrhosisDocument6 pagesCase Study Liver CirrhosisAngelica Barcelona Yumang67% (3)
- Cholecystitis Case PresDocument103 pagesCholecystitis Case PresAnton LaurencianaNo ratings yet
- A Case Study On Chronic Renal DiseaseDocument17 pagesA Case Study On Chronic Renal Diseasematucojulio100% (1)
- In Partial Fulfillment of Our Requirements IN Related Learning ExperienceDocument32 pagesIn Partial Fulfillment of Our Requirements IN Related Learning Experiencedolly joy100% (4)
- Pathophysiology - ESRDDocument5 pagesPathophysiology - ESRDheiyu100% (3)
- End - Stage Renal DiseaseDocument59 pagesEnd - Stage Renal DiseaseJonathan Diaz93% (15)
- Cirrhosis of LiverDocument7 pagesCirrhosis of LivermOHAN.S100% (2)
- Case Study CholelithiasisDocument14 pagesCase Study Cholelithiasisb_faye20No ratings yet
- Anatomy and Physiology-Liver CirrhosisDocument2 pagesAnatomy and Physiology-Liver CirrhosisHilmi Ramos100% (3)
- CASE STUDY ON ACUTE Renal FailureDocument38 pagesCASE STUDY ON ACUTE Renal FailureOdey Godwin100% (1)
- Liver Cirrhosis CaseDocument8 pagesLiver Cirrhosis Casemarlx5No ratings yet
- Liver Cirrhosis PathophysiologyDocument1 pageLiver Cirrhosis PathophysiologyCaren ReyesNo ratings yet
- Case Study CholecystitisDocument27 pagesCase Study Cholecystitismeed0290% (10)
- Chronic Gastritis Case StudyDocument17 pagesChronic Gastritis Case StudyErmawati ErmaNo ratings yet
- Case StudyDocument18 pagesCase StudyJerome GonezNo ratings yet
- Liver CirrhosisDocument5 pagesLiver CirrhosisRLLTNo ratings yet
- Colon Cancer Case StudyDocument18 pagesColon Cancer Case Studyapi-271062060100% (2)
- Case Study On Alcoholic Liver DiseaseDocument20 pagesCase Study On Alcoholic Liver DiseaseHomework PingNo ratings yet
- Case Study CKD DM Type 2Document7 pagesCase Study CKD DM Type 2Brian Cornel0% (3)
- Congestive Heart Failure. Case Study ExplanationDocument6 pagesCongestive Heart Failure. Case Study ExplanationOkenabirhie100% (1)
- Congestive Heart FailureDocument18 pagesCongestive Heart FailureAisha Rashed100% (1)
- Case Study of A Patient With Ischemic CardiomyopathyDocument33 pagesCase Study of A Patient With Ischemic Cardiomyopathyromeo rivera80% (5)
- Case Study On End Stage Renal FailureDocument19 pagesCase Study On End Stage Renal Failurelenecarglbn100% (1)
- Congestive Heart FailureDocument8 pagesCongestive Heart Failureiancel_038893% (27)
- Case Study (ACS)Document12 pagesCase Study (ACS)Kristel Joy Cabarrubias Acena100% (1)
- Cholecystitis Case StudyDocument104 pagesCholecystitis Case StudyJoshua Agawin50% (2)
- A Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and MidwiferyDocument13 pagesA Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and Midwiferyhsiria100% (2)
- Pathophysiology in Liver CirrhosisDocument4 pagesPathophysiology in Liver CirrhosisCyrus Ortalla RobinNo ratings yet
- Obstructive JaundiceDocument54 pagesObstructive JaundiceJenine Ezra M. Conol50% (2)
- A Case Study On Colon MassDocument29 pagesA Case Study On Colon MassDahlia D. SuelloNo ratings yet
- Group-1b Myocardial InfarctionDocument39 pagesGroup-1b Myocardial InfarctionJean ReyesNo ratings yet
- Pathophysiology of Liver CirrhosisDocument2 pagesPathophysiology of Liver Cirrhosisgaelty100% (4)
- The Pathology of Congestive Heart FailureDocument4 pagesThe Pathology of Congestive Heart FailureMar Ble50% (2)
- Acute Myocardial InfarctionDocument35 pagesAcute Myocardial Infarctionvirnzrobz80% (10)
- Grand Case PresentationDocument50 pagesGrand Case PresentationJean Michelle100% (1)
- Case Study Cirrhosis of LiverDocument26 pagesCase Study Cirrhosis of LiverMonika Seervi100% (1)
- 2 Acute CholecystitisDocument21 pages2 Acute CholecystitisEtteh MaryNo ratings yet
- CP Calculous-CholeDocument105 pagesCP Calculous-CholeNicole OrtegaNo ratings yet
- Liver CirrhosisDocument20 pagesLiver CirrhosischinNo ratings yet
- Case Study - MyomaDocument54 pagesCase Study - Myomauvinr100% (1)
- Liver CirrhosisDocument60 pagesLiver CirrhosisCamilla Zharine P. BantaNo ratings yet
- CP On Calculous CholelithiasisDocument102 pagesCP On Calculous Cholelithiasiskathy100% (3)
- Liver CirrhosisDocument30 pagesLiver CirrhosisMelody PardilloNo ratings yet
- Inguinal Hernia: Related Learning ExperienceDocument29 pagesInguinal Hernia: Related Learning Experience'mYk FavilaNo ratings yet
- A Family Case Study Presented To The College of NursingDocument67 pagesA Family Case Study Presented To The College of NursingShiara Ruth EdrosoloNo ratings yet
- Infection and ImmunityDocument5 pagesInfection and ImmunityBeRnAlieNo ratings yet
- Schistosomiasis, Neglected Tropical Diseases and Climate ChangeDocument2 pagesSchistosomiasis, Neglected Tropical Diseases and Climate ChangeBeRnAlieNo ratings yet
- Health Teaching: Health Perception and MaintenanceDocument7 pagesHealth Teaching: Health Perception and MaintenanceBeRnAlieNo ratings yet
- Nursing TheoriesDocument4 pagesNursing TheoriesBeRnAlieNo ratings yet
- Bach Prelude #1 - 1 3 5 8 10 5 8 10 - 1 3 5 8 10 5 8 10 - 1 2 6 9 11 6 9 11 - 1 2 6 9 11 6 9 11Document1 pageBach Prelude #1 - 1 3 5 8 10 5 8 10 - 1 3 5 8 10 5 8 10 - 1 2 6 9 11 6 9 11 - 1 2 6 9 11 6 9 11BeRnAlieNo ratings yet
- Drug StudyDocument4 pagesDrug StudyBeRnAlieNo ratings yet
- Health TeachingDocument1 pageHealth TeachingBeRnAlieNo ratings yet
- SchistosomiasisDocument3 pagesSchistosomiasisBeRnAlieNo ratings yet
- Chapel Service: January 16, 2012 Speaker: Dean Edna O. ImperialDocument12 pagesChapel Service: January 16, 2012 Speaker: Dean Edna O. ImperialBeRnAlieNo ratings yet
- Medication Sheet AuditDocument2 pagesMedication Sheet AuditBeRnAlieNo ratings yet
- Propylthiouracil (PTU)Document2 pagesPropylthiouracil (PTU)BeRnAlieNo ratings yet
- Two Way AnovaDocument2 pagesTwo Way AnovaBeRnAlieNo ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologyBeRnAlieNo ratings yet
- Propylthiouracil (PTU)Document2 pagesPropylthiouracil (PTU)BeRnAlieNo ratings yet
- Beta Met Has OneDocument5 pagesBeta Met Has Oneapi-3797941No ratings yet
- Ate - Ad.Hrr ( ("Urls": ,"segments": ,"Loc":"Mdawmdbbu1Bimdaxotq1Mzaxmdawmdawmdaw VG ") )Document1 pageAte - Ad.Hrr ( ("Urls": ,"segments": ,"Loc":"Mdawmdbbu1Bimdaxotq1Mzaxmdawmdawmdaw VG ") )BeRnAlieNo ratings yet
- Laboratory ResultsDocument2 pagesLaboratory ResultsBeRnAlieNo ratings yet
- Beta Met Has OneDocument5 pagesBeta Met Has Oneapi-3797941No ratings yet
- Brand NameDocument2 pagesBrand NameBeRnAlieNo ratings yet
- Datasheet Ark XH Battery System EngDocument2 pagesDatasheet Ark XH Battery System EngLisa CowenNo ratings yet
- ST 36Document4 pagesST 36ray72roNo ratings yet
- Chemistry Notes: SUBJECT: Leaving Cert Chemistry Level: TEACHER: Tara LyonsDocument5 pagesChemistry Notes: SUBJECT: Leaving Cert Chemistry Level: TEACHER: Tara LyonsSevinc NuriyevaNo ratings yet
- RUKUS April 2011Document40 pagesRUKUS April 2011RUKUS Magazine100% (2)
- Report - IvatanDocument28 pagesReport - IvatanJohara Winel PerezNo ratings yet
- Serial Analysis of Gene Expression (SAGE)Document34 pagesSerial Analysis of Gene Expression (SAGE)Rohit PhalakNo ratings yet
- Trends in FoodDocument3 pagesTrends in FoodAliNo ratings yet
- SCIENCEEEEEDocument3 pagesSCIENCEEEEEChristmae MaganteNo ratings yet
- Tran-Effects of Assisted JumpingDocument5 pagesTran-Effects of Assisted JumpingyoungjessNo ratings yet
- Pineapple in JohorDocument6 pagesPineapple in JohorHaiqal AzizNo ratings yet
- 10th Aug. 2011 Structural Calculation (For Sub.) - 03Document29 pages10th Aug. 2011 Structural Calculation (For Sub.) - 03Nguyễn Tiến Việt100% (1)
- Armor MagazineDocument32 pagesArmor Magazine"Rufus"100% (1)
- 40 RT-flex Control-System Rev01Document68 pages40 RT-flex Control-System Rev01Mayvon Botelho100% (2)
- LJ-V7080 DatasheetDocument2 pagesLJ-V7080 DatasheetOrhan DenizliNo ratings yet
- Easergy PS100 48VDC Power SupplyDocument2 pagesEasergy PS100 48VDC Power SupplyRichard SyNo ratings yet
- Energy Transfer in Cell During Exercise and Oxygen Metabolism and Transport - PalakDocument85 pagesEnergy Transfer in Cell During Exercise and Oxygen Metabolism and Transport - Palakpalooo4No ratings yet
- Navy Supplement To The DOD Dictionary of Military and Associated Terms, 2011Document405 pagesNavy Supplement To The DOD Dictionary of Military and Associated Terms, 2011bateljupko100% (1)
- MioPocket ReadmeDocument30 pagesMioPocket Readmelion78No ratings yet
- Typical Section SC 10: Kerajaan MalaysiaDocument1 pageTypical Section SC 10: Kerajaan MalaysiaAisyah Atiqah KhalidNo ratings yet
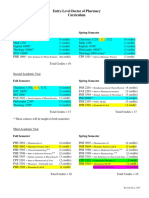
- Pharmd CurriculumDocument18 pagesPharmd Curriculum5377773No ratings yet
- (Eng) Zx890lch 5a Ks En316Document13 pages(Eng) Zx890lch 5a Ks En316MC TAK LEENo ratings yet
- Thermoplastic Tubing: Catalogue 5210/UKDocument15 pagesThermoplastic Tubing: Catalogue 5210/UKGeo BuzatuNo ratings yet
- Index PDFDocument159 pagesIndex PDFHüseyin IşlakNo ratings yet
- Module in Pe 103Document79 pagesModule in Pe 103Kym Dacudao100% (1)
- Intro Slow Keyofg: Em7 G5 A7Sus4 G C/G D/F# AmDocument2 pagesIntro Slow Keyofg: Em7 G5 A7Sus4 G C/G D/F# Ammlefev100% (1)
- Academic Reading: All Answers Must Be Written On The Answer SheetDocument21 pagesAcademic Reading: All Answers Must Be Written On The Answer SheetLemon MahamudNo ratings yet
- E-OLSS: Electronic ControlDocument12 pagesE-OLSS: Electronic ControlSamidiNo ratings yet
- Dizziness - Vertigo and HomoeopathyDocument38 pagesDizziness - Vertigo and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- John Sisler CISSP Study GuideDocument126 pagesJohn Sisler CISSP Study GuideAnthonyNo ratings yet
- Bahir Dar University BIT: Faculity of Mechanical and Industrial EngineeringDocument13 pagesBahir Dar University BIT: Faculity of Mechanical and Industrial Engineeringfraol girmaNo ratings yet
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- A Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentFrom EverandA Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentNo ratings yet
- Brain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensFrom EverandBrain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensRating: 5 out of 5 stars5/5 (2)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- I Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionFrom EverandI Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionRating: 4 out of 5 stars4/5 (74)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackFrom EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackRating: 4.5 out of 5 stars4.5/5 (152)
- I Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionFrom EverandI Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionRating: 4.5 out of 5 stars4.5/5 (106)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)