You might also like
- War crimes and crimes against humanity in the Rome Statute of the International Criminal CourtFrom EverandWar crimes and crimes against humanity in the Rome Statute of the International Criminal CourtNo ratings yet
- Rules on execution, satisfaction and effects of judgmentsDocument13 pagesRules on execution, satisfaction and effects of judgmentsJennifer KnowlesNo ratings yet
- Damaso CaseDocument27 pagesDamaso CaseKC Barras100% (1)
- Legal Memorandum SamplaDocument4 pagesLegal Memorandum SamplaCalvin Canlas SardiaNo ratings yet
- LBC Loan AgreementDocument5 pagesLBC Loan AgreementDennis Aran Tupaz AbrilNo ratings yet
- July 6 Ra 11223 Reji JewelDocument25 pagesJuly 6 Ra 11223 Reji JewelHomura Ch.No ratings yet
- CDIF Nfa MoaDocument18 pagesCDIF Nfa MoakarlajoannaNo ratings yet
- Solicitation Letter 1Document1 pageSolicitation Letter 1dNo ratings yet
- Hello! Cupcake Partnership AgreementDocument4 pagesHello! Cupcake Partnership AgreementAnn Camille JoaquinNo ratings yet
- PCO Training Category A - Training Schedule - 2018.06 - GREEN CorpDocument2 pagesPCO Training Category A - Training Schedule - 2018.06 - GREEN CorpMarcus TandaanNo ratings yet
- Dental Clinic AgreementDocument9 pagesDental Clinic AgreementAnwarNo ratings yet
- Bangsamoro ORGANIC Law: What You Need To Know: Atty. Carizza Joy Y. GonzalesDocument68 pagesBangsamoro ORGANIC Law: What You Need To Know: Atty. Carizza Joy Y. GonzalesSalman Dimaporo RashidNo ratings yet
- Contract To Sell - AuDocument4 pagesContract To Sell - AuMARIA SANDRA SalvadorNo ratings yet
- Vice Mayor CreedDocument1 pageVice Mayor CreedYes Tirol DumaganNo ratings yet
- Affidavit of Loss: Republic of The Philippines) Done: City of Baguio) SsDocument1 pageAffidavit of Loss: Republic of The Philippines) Done: City of Baguio) SsAmanda HernandezNo ratings yet
- Sandiganbayan Ruling On Ninoy AssassinationDocument184 pagesSandiganbayan Ruling On Ninoy AssassinationRaul A. ArcangelNo ratings yet
- LEGFORM - Assignment of SalaryDocument1 pageLEGFORM - Assignment of SalaryRaymarc Elizer AsuncionNo ratings yet
- Employment Contract Template 1414717815774Document5 pagesEmployment Contract Template 1414717815774Santee HaylesNo ratings yet
- PD 1829 Obstruction of Justice PDFDocument1 pagePD 1829 Obstruction of Justice PDFtoshkenbergNo ratings yet
- Template Memorandum of UnderstandingDocument4 pagesTemplate Memorandum of Understandingkb gagsNo ratings yet
- Payment Guaranty: Between: (CREDITOR NAME) (The "Creditor"), A Corporation Organized and ExistingDocument6 pagesPayment Guaranty: Between: (CREDITOR NAME) (The "Creditor"), A Corporation Organized and ExistingYushardianto Eka PutraNo ratings yet
- Legal Memorandum Psychological Incapacity Petitioner - Google SearchDocument2 pagesLegal Memorandum Psychological Incapacity Petitioner - Google SearchSarah Jane-Shae O. Semblante0% (1)
- Bus Company Liable for Fatal AccidentDocument39 pagesBus Company Liable for Fatal AccidentAnn Catalan0% (1)
- Demand Letter (Mano Biboy)Document1 pageDemand Letter (Mano Biboy)v_sharonNo ratings yet
- Visa Services AgreementDocument3 pagesVisa Services Agreementtitus72140No ratings yet
- 2015 2016 Tax Case Digest PDFDocument114 pages2015 2016 Tax Case Digest PDFAnonymous CWcXthhZgxNo ratings yet
- Woodhouse Vs HaliliDocument2 pagesWoodhouse Vs Halilicyndigrace_mNo ratings yet
- Consent of Action by Directors in Lieu of Organizational MeetingsDocument22 pagesConsent of Action by Directors in Lieu of Organizational MeetingsDiego AntoliniNo ratings yet
- Dear PAO - AdoptionDocument2 pagesDear PAO - AdoptionEdison FloresNo ratings yet
- Menzi and Co. v. BastidaDocument1 pageMenzi and Co. v. BastidaBless CarpenaNo ratings yet
- GILAT Satellite Vs UCPBDocument8 pagesGILAT Satellite Vs UCPBGloria Diana Dulnuan0% (1)
- Jacob vs. CA - 224 S 189Document2 pagesJacob vs. CA - 224 S 189Zesyl Avigail FranciscoNo ratings yet
- Consent For Participation To PhieDocument1 pageConsent For Participation To PhiebenNo ratings yet
- A.M. No. 03-1-09-SCDocument8 pagesA.M. No. 03-1-09-SCFelora MangawangNo ratings yet
- LTD Cases Last PartDocument4 pagesLTD Cases Last PartlexxNo ratings yet
- POLIREV Case Doctrines 2Document128 pagesPOLIREV Case Doctrines 2Thirdee Dapal100% (1)
- 1, Petition To COMELECDocument47 pages1, Petition To COMELECMCamelloNo ratings yet
- Irr Republic Act No. 11642, June 28, 2022Document60 pagesIrr Republic Act No. 11642, June 28, 2022Martin OcampoNo ratings yet
- Philippine foreign debt amid COVID-19Document2 pagesPhilippine foreign debt amid COVID-19James ReaNo ratings yet
- TAXATION OF FOREIGN INDIVIDUALS IN THE PHILIPPINESDocument25 pagesTAXATION OF FOREIGN INDIVIDUALS IN THE PHILIPPINESHailin QuintosNo ratings yet
- PhilHealth: A Brief OverviewDocument31 pagesPhilHealth: A Brief OverviewAngelica Mojica LaroyaNo ratings yet
- Villaruel Vs Manila Motor CorpDocument11 pagesVillaruel Vs Manila Motor CorpRachelle DomingoNo ratings yet
- Results and Discussion InsightsDocument9 pagesResults and Discussion InsightsBeaNo ratings yet
- Demand Letter For BP 22Document1 pageDemand Letter For BP 22Json GalvezNo ratings yet
- Contract of ServiceDocument15 pagesContract of ServiceMaylyn Laranjo-Nazareno VillamorNo ratings yet
- Cta 2D CV 08551 M 2016mar02 AssDocument10 pagesCta 2D CV 08551 M 2016mar02 AssKathrine Chin LuNo ratings yet
- PHILHEALTHDocument17 pagesPHILHEALTHMariaMonicaNo ratings yet
- TRANSCRIPT: 6th Public Hearing of The Senate Blue Ribbon Committee On The $81-M Money Laundering CaseDocument172 pagesTRANSCRIPT: 6th Public Hearing of The Senate Blue Ribbon Committee On The $81-M Money Laundering CaseBlogWatchNo ratings yet
- Dipatuan Vs MangotaraDocument10 pagesDipatuan Vs MangotaraBorgy AmbuloNo ratings yet
- Case Digest On Concealment: Insurance LawDocument10 pagesCase Digest On Concealment: Insurance LawRaq KhoNo ratings yet
- People vs. GuillenDocument4 pagesPeople vs. GuillensakuraNo ratings yet
- (G.R. No. 170007. April 7, 2014.) Tabangao Shell Refinery Employees Association, Petitioner, vs. Pilipinas Shell Petroleum CORPORATION, RespondentDocument3 pages(G.R. No. 170007. April 7, 2014.) Tabangao Shell Refinery Employees Association, Petitioner, vs. Pilipinas Shell Petroleum CORPORATION, RespondentEkie Gonzaga100% (1)
- 43E - CIR vs. Philippine American LIfe InsuranceDocument3 pages43E - CIR vs. Philippine American LIfe InsuranceDannaIngaranNo ratings yet
- Syllabus PALEDocument6 pagesSyllabus PALEJohayrah CampongNo ratings yet
- Guarantor rights and obligations between debtor and creditorDocument10 pagesGuarantor rights and obligations between debtor and creditormichaelargabiosoNo ratings yet
- UP Alumni Update FormDocument6 pagesUP Alumni Update Formjpag000100% (1)
- Deed of Absolute Sale - SyjuecoDocument6 pagesDeed of Absolute Sale - SyjuecoCristopher ReyesNo ratings yet
- Sunlife Assurance Company Vs CADocument2 pagesSunlife Assurance Company Vs CApaul2574No ratings yet
- General principles of remedial lawDocument207 pagesGeneral principles of remedial lawchey_anneNo ratings yet
- Portland Couples Therapy Consent To Treatment Fee Agreement - New Leaves ClinicDocument6 pagesPortland Couples Therapy Consent To Treatment Fee Agreement - New Leaves ClinicavacarterNo ratings yet
- Medical History PDFDocument1 pageMedical History PDFKidsStopDentalNo ratings yet
- Kids Stop Dental Notice of PrivacyDocument2 pagesKids Stop Dental Notice of PrivacyKidsStopDentalNo ratings yet
- KSD Patient RegistrationDocument1 pageKSD Patient RegistrationKidsStopDentalNo ratings yet
- Medical Release Authorization Form For MinorsDocument1 pageMedical Release Authorization Form For MinorsKidsStopDentalNo ratings yet
- Kids Stop Dental Notice of PrivacyDocument2 pagesKids Stop Dental Notice of PrivacyKidsStopDentalNo ratings yet
- Bentone 30 Msds (Eu-Be)Document6 pagesBentone 30 Msds (Eu-Be)Amir Ososs0% (1)
- Compressive Strength Beam DesignDocument70 pagesCompressive Strength Beam DesignDjuned0% (1)
- Yamaha Nmax 155 - To Turn The Vehicle Power OffDocument1 pageYamaha Nmax 155 - To Turn The Vehicle Power Offmotley crewzNo ratings yet
- E2 PTAct 9 7 1 DirectionsDocument4 pagesE2 PTAct 9 7 1 DirectionsEmzy SorianoNo ratings yet
- Gattu Madhuri's Resume for ECE GraduateDocument4 pagesGattu Madhuri's Resume for ECE Graduatedeepakk_alpineNo ratings yet
- Econ Old Test 2Document7 pagesEcon Old Test 2Homer ViningNo ratings yet
- 2020-05-14 County Times NewspaperDocument32 pages2020-05-14 County Times NewspaperSouthern Maryland OnlineNo ratings yet
- Wind EnergyDocument6 pagesWind Energyshadan ameenNo ratings yet
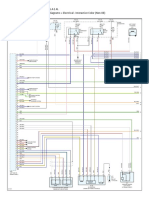
- Engine Controls (Powertrain Management) - ALLDATA RepairDocument4 pagesEngine Controls (Powertrain Management) - ALLDATA Repairmemo velascoNo ratings yet
- Distribution of Laptop (Ha-Meem Textiles Zone)Document3 pagesDistribution of Laptop (Ha-Meem Textiles Zone)Begum Nazmun Nahar Juthi MozumderNo ratings yet
- EFM2e, CH 03, SlidesDocument36 pagesEFM2e, CH 03, SlidesEricLiangtoNo ratings yet
- CTS experiments comparisonDocument2 pagesCTS experiments comparisonmanojkumarNo ratings yet
- Law of TortsDocument22 pagesLaw of TortsRadha KrishanNo ratings yet
- 5.0 A Throttle Control H-BridgeDocument26 pages5.0 A Throttle Control H-Bridgerumellemur59No ratings yet
- Applicants at Huye Campus SiteDocument4 pagesApplicants at Huye Campus SiteHIRWA Cyuzuzo CedricNo ratings yet
- Sop EcuDocument11 pagesSop Ecuahmed saeedNo ratings yet
- PNB - Recruitment For The Post of Chief Security OfficerDocument3 pagesPNB - Recruitment For The Post of Chief Security OfficerCareerNotifications.comNo ratings yet
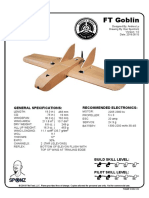
- FT Goblin Full SizeDocument7 pagesFT Goblin Full SizeDeakon Frost100% (1)
- Overall Dimensions and Mounting: Solar Water Pump Controller Mu - G3 Solar Mu - G5 Solar Mu - G7.5 Solar Mu - G10 SolarDocument2 pagesOverall Dimensions and Mounting: Solar Water Pump Controller Mu - G3 Solar Mu - G5 Solar Mu - G7.5 Solar Mu - G10 SolarVishak ThebossNo ratings yet
- Lorilie Muring ResumeDocument1 pageLorilie Muring ResumeEzekiel Jake Del MundoNo ratings yet
- Indian Institute of Management KozhikodeDocument5 pagesIndian Institute of Management KozhikodepranaliNo ratings yet
- Railway RRB Group D Book PDFDocument368 pagesRailway RRB Group D Book PDFAshish mishraNo ratings yet
- Binaural Recording Technology: A Historical Review and Possible Future DevelopmentsDocument22 pagesBinaural Recording Technology: A Historical Review and Possible Future DevelopmentsNery BorgesNo ratings yet
- Fundamentals of Marketing NotebookDocument24 pagesFundamentals of Marketing NotebookMorrisa AlexanderNo ratings yet
- Gary Mole and Glacial Energy FraudDocument18 pagesGary Mole and Glacial Energy Fraudskyy22990% (1)
- Elementary School: Cash Disbursements RegisterDocument1 pageElementary School: Cash Disbursements RegisterRonilo DagumampanNo ratings yet
- Notes On Lesson: Faculty Name Code Subject Name CodeDocument108 pagesNotes On Lesson: Faculty Name Code Subject Name CodeJeba ChristoNo ratings yet
- Supply Chain ManagementDocument30 pagesSupply Chain ManagementSanchit SinghalNo ratings yet
- Super Flexible, Super Fast, Super Value: Gigabit PTMP Client and PTP With Modular AntennasDocument5 pagesSuper Flexible, Super Fast, Super Value: Gigabit PTMP Client and PTP With Modular AntennasAbdallaNo ratings yet
- I. ICT (Information & Communication Technology: LESSON 1: Introduction To ICTDocument2 pagesI. ICT (Information & Communication Technology: LESSON 1: Introduction To ICTEissa May VillanuevaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityFrom EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityRating: 4.5 out of 5 stars4.5/5 (109)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)