You might also like
- Inverse LaplaceDocument12 pagesInverse LaplaceΜΙΚΕ ΖΥΡNo ratings yet
- Lecture Fourier TransformDocument24 pagesLecture Fourier TransformML NarasimhamNo ratings yet
- Assignment 1Document2 pagesAssignment 1ashmitashrivasNo ratings yet
- Example of AliasingDocument1 pageExample of AliasingashmitashrivasNo ratings yet
- Git Cheat Sheet NotesDocument2 pagesGit Cheat Sheet NotesashmitashrivasNo ratings yet
- Airborne InternetDocument27 pagesAirborne InternetashmitashrivasNo ratings yet
- RVR Institute of Engineering & Technology: ECE DepartmentDocument33 pagesRVR Institute of Engineering & Technology: ECE DepartmentashmitashrivasNo ratings yet
- Example of AliasingDocument1 pageExample of AliasingashmitashrivasNo ratings yet
- Six SenseDocument7 pagesSix SenseashmitashrivasNo ratings yet
- Boy Goes BallisticDocument1 pageBoy Goes BallisticashmitashrivasNo ratings yet
- Multiple Choice Questions Organized by Freller Chapter 11 The Industrial Society and The Struggle For Reform 1815-1850Document40 pagesMultiple Choice Questions Organized by Freller Chapter 11 The Industrial Society and The Struggle For Reform 1815-1850ashmitashrivasNo ratings yet
- Obligations and Contracts Legal NotesDocument25 pagesObligations and Contracts Legal NotesashmitashrivasNo ratings yet
- Winston ChurchillDocument1 pageWinston ChurchillashmitashrivasNo ratings yet
- Schemekerala University B Tech Computer Science SyllabusDocument103 pagesSchemekerala University B Tech Computer Science SyllabusAbhijith MarathakamNo ratings yet
- Git Cheat Sheet NotesDocument2 pagesGit Cheat Sheet NotesashmitashrivasNo ratings yet
- LatitudeDocument2 pagesLatitudeJosé Ignacio Aparicio MéndezNo ratings yet
- Operation & Maintenance Best Practice O&MBestPracticesDocument169 pagesOperation & Maintenance Best Practice O&MBestPracticesevrimkNo ratings yet
- Btech Kerala University It2008 SchemeDocument82 pagesBtech Kerala University It2008 SchemeDenver KuNo ratings yet
- Inventory Management: Ravindra S. GokhaleDocument58 pagesInventory Management: Ravindra S. GokhaleAmrita PrasadNo ratings yet
- Job VacanciesDocument1 pageJob VacanciesashmitashrivasNo ratings yet
- Sbi Po Advt Jan-2013Document3 pagesSbi Po Advt Jan-2013api-193985166No ratings yet
- Mein Kampf - My Struggle - Unexpurgated Ed - Adolf HitlerDocument1,501 pagesMein Kampf - My Struggle - Unexpurgated Ed - Adolf Hitlerkabplop88% (8)
- Mark Twain Quote: Luck Happens When Preparation Meets OpportunityDocument1 pageMark Twain Quote: Luck Happens When Preparation Meets OpportunityashmitashrivasNo ratings yet
- COSMOS Chapter 11 Solution 109Document1 pageCOSMOS Chapter 11 Solution 109ashmitashrivasNo ratings yet
- Fci SyllabusDocument3 pagesFci SyllabusNeha GogiaNo ratings yet
- At Command Set For Nokia GSM and WCDMA Products v1 2 enDocument111 pagesAt Command Set For Nokia GSM and WCDMA Products v1 2 endhwanil_k8031No ratings yet
- Inventory Management-OutlineDocument31 pagesInventory Management-OutlineashmitashrivasNo ratings yet
- At Command Set For Nokia GSM and WCDMA Products v1 2 enDocument111 pagesAt Command Set For Nokia GSM and WCDMA Products v1 2 endhwanil_k8031No ratings yet
- LatitudeDocument2 pagesLatitudeJosé Ignacio Aparicio MéndezNo ratings yet
- 1 EX ST 411/611 Homework 3Document7 pages1 EX ST 411/611 Homework 3ashmitashrivasNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cyber Crimes and Frauds, Cyber Laws, Types and Tools of HackingDocument25 pagesCyber Crimes and Frauds, Cyber Laws, Types and Tools of HackingKishan Kumar SharmaNo ratings yet
- Data Logger Geokon Linear CoefficientsDocument6 pagesData Logger Geokon Linear Coefficientscchung147554No ratings yet
- FPGA Implementation of 2D-DCT For Image CompressionDocument4 pagesFPGA Implementation of 2D-DCT For Image CompressionVeronica GeorgeNo ratings yet
- MDaemon Mail Server Installation Guide Amirz ComDocument19 pagesMDaemon Mail Server Installation Guide Amirz ComAdhys SmanSa100% (1)
- Final Presentation BANK OF BARODA 1Document8 pagesFinal Presentation BANK OF BARODA 1Pooja GoyalNo ratings yet
- Performance of LDPC Codes For SatelliteDocument4 pagesPerformance of LDPC Codes For SatelliteMohamed MydeenNo ratings yet
- 9 - USART - EEPROM - CCP - Realtime Applications PDFDocument57 pages9 - USART - EEPROM - CCP - Realtime Applications PDFSrujan KazipetaNo ratings yet
- Opl 3 DatabaseDocument19 pagesOpl 3 Databasedeep_sorari7No ratings yet
- NI TutorialDocument3 pagesNI TutorialMuhammad IsrarNo ratings yet
- Summer Matlab Exam SolutionDocument5 pagesSummer Matlab Exam SolutionGrifinaNuzuliaNo ratings yet
- Sample - Customer Churn Prediction Python DocumentationDocument33 pagesSample - Customer Churn Prediction Python Documentationchandrakanth BNo ratings yet
- Oracle9: Database Generic Documentation Master IndexDocument734 pagesOracle9: Database Generic Documentation Master Indexhiiam6cNo ratings yet
- Error Message Reference: Oracle® Hyperion Calculation ManagerDocument4 pagesError Message Reference: Oracle® Hyperion Calculation Managermess lionNo ratings yet
- Function Generator Using X86 MicroprocessorDocument7 pagesFunction Generator Using X86 Microprocessormmorsy1981No ratings yet
- 02 Q8 9 10 TogetherDocument21 pages02 Q8 9 10 TogethermlaorrcNo ratings yet
- Microsoft Exchange Server Version 5.5 Service Pack 3 Information inDocument4 pagesMicrosoft Exchange Server Version 5.5 Service Pack 3 Information inacky30No ratings yet
- BSC It - Sem IV - Core JavaDocument141 pagesBSC It - Sem IV - Core JavaValia Centre of ExcellenceNo ratings yet
- TLEDocument26 pagesTLEDazzle Lanuzo EsquejoNo ratings yet
- Deepsoil User Manual v6 PDFDocument116 pagesDeepsoil User Manual v6 PDFARVINDNo ratings yet
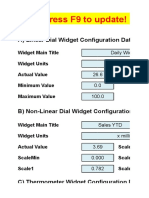
- Excel Dashboard WidgetsDocument47 pagesExcel Dashboard WidgetskhincowNo ratings yet
- BOMBER A Tool For Estimating Water Quali PDFDocument6 pagesBOMBER A Tool For Estimating Water Quali PDFaubrey mae VargasNo ratings yet
- ANA Sales Enablement FrameworkDocument1 pageANA Sales Enablement FrameworkDemand Metric100% (1)
- High-Performance Cluster Configurations For ANSYS Fluid DynamicsDocument36 pagesHigh-Performance Cluster Configurations For ANSYS Fluid DynamicsVyssionNo ratings yet
- Assignment 4 Client ServerDocument5 pagesAssignment 4 Client ServerClip-part CollectionsNo ratings yet
- Grcka I Srpska Prosveta Vladan DjordjevicDocument293 pagesGrcka I Srpska Prosveta Vladan DjordjevicBorisSubNo ratings yet
- SamsungDocument5 pagesSamsungjcg41263No ratings yet
- Control Lab Experiment 2Document3 pagesControl Lab Experiment 2AnasElgaoodNo ratings yet
- Jupiter Rising: A Decade of Clos Topologies and Centralized Control in Google's Datacenter NetworkDocument10 pagesJupiter Rising: A Decade of Clos Topologies and Centralized Control in Google's Datacenter Networkthsilva85No ratings yet
- CV Wira DharmaDocument2 pagesCV Wira DharmaRegino Agustri BeckerNo ratings yet
- TifrDocument3 pagesTifrgrasheedNo ratings yet