You might also like
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Nephrolithiasis CPDocument54 pagesNephrolithiasis CPSheena VallesNo ratings yet
- Acute PyelonephritisDocument24 pagesAcute Pyelonephritismayey22100% (3)
- Nursing Case AuditDocument53 pagesNursing Case AuditJhean MeansNo ratings yet
- Obstructive Uropathy Case StudyDocument19 pagesObstructive Uropathy Case StudyNayan MaharjanNo ratings yet
- CHOLECYSTECTOMYDocument35 pagesCHOLECYSTECTOMYfaitheee100% (3)
- Case Study On Bilateral NephrolithiasisDocument84 pagesCase Study On Bilateral NephrolithiasisSteph BulanNo ratings yet
- CholelithiasisDocument6 pagesCholelithiasismarkzamNo ratings yet
- A Case Study On A Patient Diagnosed With UlcerDocument20 pagesA Case Study On A Patient Diagnosed With UlcerNevoj_Nygrin_3313No ratings yet
- Obstructive Uropathy: Nitha. K 2 Year MSC NursingDocument67 pagesObstructive Uropathy: Nitha. K 2 Year MSC NursingNITHA KNo ratings yet
- Acute PyelonephritisDocument59 pagesAcute PyelonephritisKylie Golindang100% (1)
- Bladder Cancer: By: Estigoy, Harriet and Galang, Cuttie AnneDocument18 pagesBladder Cancer: By: Estigoy, Harriet and Galang, Cuttie AnneCuttie Anne Galang100% (1)
- CellulitisDocument16 pagesCellulitisMhOt AmAd100% (1)
- Drug Study FDocument3 pagesDrug Study FFatima Love Ariate-ArcasetasNo ratings yet
- Anatomy and Physiology of The GallbladderDocument1 pageAnatomy and Physiology of The GallbladderRojanisa Baculi RomathoNo ratings yet
- Pernicious AnemiaDocument7 pagesPernicious AnemiaTracy PearlNo ratings yet
- 2 Acute CholecystitisDocument21 pages2 Acute CholecystitisEtteh MaryNo ratings yet
- NCP OsteosarcomaDocument6 pagesNCP OsteosarcomaNiksNo ratings yet
- Ugib Case StudyDocument30 pagesUgib Case StudyVenus Glaze Verzola80% (5)
- CystolithiasisDocument7 pagesCystolithiasisRaul Nocete100% (1)
- Module V ActDocument3 pagesModule V ActQueencess hayoNo ratings yet
- Obstructive UropathyDocument8 pagesObstructive UropathyTeslim Raji100% (1)
- Case Study About Rectal CADocument11 pagesCase Study About Rectal CACantiga Vhadz0% (1)
- Date Physician's Order RationaleDocument4 pagesDate Physician's Order RationaleJerremy LuqueNo ratings yet
- Liver CirrhosisDocument60 pagesLiver CirrhosisCamilla Zharine P. BantaNo ratings yet
- Liver AbscessDocument3 pagesLiver AbscessStephanie Pe100% (1)
- Regular Insulin: A Drug Study OnDocument9 pagesRegular Insulin: A Drug Study OnSophia IbuyanNo ratings yet
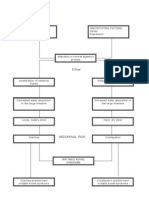
- Pathophysiology (Client Base) :: Predisposing Factors: Precipitating FactorsDocument1 pagePathophysiology (Client Base) :: Predisposing Factors: Precipitating Factorsleslie_macasaetNo ratings yet
- Cholelithiasis Brief DiscussionDocument8 pagesCholelithiasis Brief Discussionriel100% (6)
- Case Analysis in CholecystectomyDocument9 pagesCase Analysis in CholecystectomyMay Ann Magdaraog ArdamilNo ratings yet
- Case Scenario Peptic UlcerDocument2 pagesCase Scenario Peptic Ulcerchetankumarbhumireddy0% (1)
- Humulin R, Novolin RDocument2 pagesHumulin R, Novolin RSheri490100% (2)
- Pancreatitis: (Alterations in Metabolic and Endocrine Functions)Document7 pagesPancreatitis: (Alterations in Metabolic and Endocrine Functions)Jorie Roco0% (1)
- CP Cholecystitis With Cholethiasis, Mild Dehydration CAPDocument181 pagesCP Cholecystitis With Cholethiasis, Mild Dehydration CAPArianna Jasmine MabungaNo ratings yet
- NephrolithiasisDocument2 pagesNephrolithiasisDeepthiNo ratings yet
- Gouty Arthritissss PathophyDocument2 pagesGouty Arthritissss Pathophybilliam123No ratings yet
- PyelonephritisDocument59 pagesPyelonephritisGheyl GabrielNo ratings yet
- Fluoracil Drug StudyDocument3 pagesFluoracil Drug StudyNicole Louize CaloraNo ratings yet
- AGE PathophysiologyDocument1 pageAGE PathophysiologyZhenmeiNo ratings yet
- Pa Tho Irritable Bowel SyndromeDocument1 pagePa Tho Irritable Bowel Syndromekaye0403No ratings yet
- Urinary Tract Infection Anatomy and PhysiologyDocument12 pagesUrinary Tract Infection Anatomy and PhysiologyPaul Anthony Centeno PimentelNo ratings yet
- CHOLELITHIASISSDocument29 pagesCHOLELITHIASISSAngelica Mercado SirotNo ratings yet
- Urinary Tract Infectio Case StudyDocument17 pagesUrinary Tract Infectio Case Studyjunex123No ratings yet
- Drug StudyDocument2 pagesDrug StudyJanina Patricia BuddleNo ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- Etiology, Pathophysiology, and Clinical Manifestations of CholecystitisDocument3 pagesEtiology, Pathophysiology, and Clinical Manifestations of CholecystitisGerriNo ratings yet
- Myoma PathoDocument3 pagesMyoma PathoJan Michael Artiaga100% (1)
- Chronic Calculous CholecystitisDocument35 pagesChronic Calculous CholecystitisJoshua AgawinNo ratings yet
- Bea-Case StudyDocument21 pagesBea-Case Studybea pegadNo ratings yet
- UGIBDocument1 pageUGIBgarrl100% (1)
- Myocardial InfarctionDocument45 pagesMyocardial InfarctionGopal SinghNo ratings yet
- Nursing Process of A Client With CholelithiasisDocument21 pagesNursing Process of A Client With Cholelithiasisapi-3822508100% (6)
- Acute PyelonephritisDocument16 pagesAcute PyelonephritisDilshan WickramanayakaNo ratings yet
- Case Study Introduction CKDDocument6 pagesCase Study Introduction CKDRhajibNo ratings yet
- Individual Case Study Acute GlomerulonephritisDocument26 pagesIndividual Case Study Acute GlomerulonephritisBatrisyia HalimsNo ratings yet
- Acute PyelonephritisDocument24 pagesAcute PyelonephritisChristine Karen Ang Suarez100% (1)
- Individual Case Study Acute GlomerulonephritisDocument26 pagesIndividual Case Study Acute GlomerulonephritisMonique ReyesNo ratings yet
- Osteosarcoma CaseDocument28 pagesOsteosarcoma CaseChristine Karen Ang SuarezNo ratings yet
- Colorectal CancerDocument50 pagesColorectal CancerHans Chester Rirao Capinding100% (2)
- Peritoneal Carcinomatosis Grand Case StudyDocument69 pagesPeritoneal Carcinomatosis Grand Case StudyBeverly Joy RubiNo ratings yet
- Pathophysiology EclampsiaDocument5 pagesPathophysiology EclampsiaChristine Karen Ang SuarezNo ratings yet
- Osteosarcoma CaseDocument28 pagesOsteosarcoma CaseChristine Karen Ang SuarezNo ratings yet
- Nursing Care PlanDocument28 pagesNursing Care PlanChristine Karen Ang Suarez67% (3)
- NCP - Diabetes Mellitus Type IIDocument10 pagesNCP - Diabetes Mellitus Type IIChristine Karen Ang SuarezNo ratings yet
- NCP Pathophysiology Acute PyelonephritisDocument20 pagesNCP Pathophysiology Acute PyelonephritisChristine Karen Ang Suarez100% (2)
- Kawasaki DiseaseDocument47 pagesKawasaki DiseaseChristine Karen Ang Suarez100% (1)
- Diabetes Mellitus Type IIDocument26 pagesDiabetes Mellitus Type IIChristine Karen Ang Suarez100% (1)
- Amoebiasis CaseDocument51 pagesAmoebiasis CaseChristine Karen Ang SuarezNo ratings yet
- Community DX 2Document8 pagesCommunity DX 2Christine Karen Ang SuarezNo ratings yet
- Breast CancerDocument53 pagesBreast CancerChristine Karen Ang Suarez100% (3)
- Acute PyelonephritisDocument24 pagesAcute PyelonephritisChristine Karen Ang Suarez100% (1)
- PathophysiologyDocument5 pagesPathophysiologyJessyl GirayNo ratings yet
- ASS - History Taking and Physical ExaminationDocument142 pagesASS - History Taking and Physical ExaminationTrixDelaCruz100% (3)
- Principles of Risk Management and Insurance 12Th Edition Rejda Test Bank Full Chapter PDFDocument34 pagesPrinciples of Risk Management and Insurance 12Th Edition Rejda Test Bank Full Chapter PDFJasonMoralesykcx100% (9)
- Body LiceDocument2 pagesBody LiceCeline BrantegemNo ratings yet
- Pulp Treatment NakabehDocument118 pagesPulp Treatment Nakabehdr_ahmad_zuhdiNo ratings yet
- WJG 27 1691Document26 pagesWJG 27 1691Valentina QuinteroNo ratings yet
- A PT With Shortness of Breath - 93355 - 284 - 20602Document3 pagesA PT With Shortness of Breath - 93355 - 284 - 20602Raju NiraulaNo ratings yet
- Cancer Case StudyDocument3 pagesCancer Case Studyapi-311163159No ratings yet
- Case of Nuclear SclerosisDocument32 pagesCase of Nuclear Sclerosismayan005No ratings yet
- 306 1164 1 PB PDFDocument6 pages306 1164 1 PB PDFDini RizkyNo ratings yet
- Bell 2010Document8 pagesBell 2010RosarioBengocheaSecoNo ratings yet
- 2 Nursing Assessment 1Document1 page2 Nursing Assessment 1Lorraine GambitoNo ratings yet
- Endocrine Part 2 DRAFTDocument6 pagesEndocrine Part 2 DRAFTPreeti Joan BuxaniNo ratings yet
- Feng ShuiDocument87 pagesFeng Shuisrce100% (2)
- MCQ 2Document12 pagesMCQ 2Zahid Mahmood RaahatNo ratings yet
- Peripheral Neuropathies in Clinical PracticeDocument398 pagesPeripheral Neuropathies in Clinical PracticeIka Gultom100% (1)
- What Is Mental Health or Emotional HealthDocument5 pagesWhat Is Mental Health or Emotional HealthAl LanNo ratings yet
- House Brackmann: Bels Palsy ScoreDocument2 pagesHouse Brackmann: Bels Palsy ScoreBaharudin Yusuf RamadhaniNo ratings yet
- AAP January 2022 Complete Issue Pediatrics in ReviewDocument71 pagesAAP January 2022 Complete Issue Pediatrics in ReviewsureshNo ratings yet
- Dated:: I Hereby Declare That The Project Titled "Effect of Brand On CustomerDocument75 pagesDated:: I Hereby Declare That The Project Titled "Effect of Brand On CustomerParshant GargNo ratings yet
- Understanding POTS - The Invisible IllnessDocument10 pagesUnderstanding POTS - The Invisible IllnessSpencer100% (1)
- Pulpotomy Pulpectomy PDFDocument1 pagePulpotomy Pulpectomy PDFShinta Syafe'iNo ratings yet
- Orchitis: Dr. Egi Edward Manuputty, Sp.UDocument26 pagesOrchitis: Dr. Egi Edward Manuputty, Sp.Uvanadiel4No ratings yet
- Final MBBS Part I Lectures Vol I PDFDocument82 pagesFinal MBBS Part I Lectures Vol I PDFHan TunNo ratings yet
- Biology Investigatory ProjectDocument17 pagesBiology Investigatory ProjectAnmol Dhungel100% (6)
- Breast Cancer PresentationDocument52 pagesBreast Cancer Presentationapi-341607639100% (1)
- MS Review Exam 5Document10 pagesMS Review Exam 5Gian Karlo GarridoNo ratings yet
- Melanoma CaseDocument4 pagesMelanoma CaseDinarkram Rabreca EculNo ratings yet
- CADDRA ADHD Information Resources HandoutDocument2 pagesCADDRA ADHD Information Resources HandoutMustafa AlmasoudiNo ratings yet
- American EskimosDocument21 pagesAmerican EskimosJorie RocoNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainFrom EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainRating: 4 out of 5 stars4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (59)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)