You might also like
- Textbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyFrom EverandTextbook of Urgent Care Management: Chapter 39, Ensuring Patient SafetyNo ratings yet
- Cardiac Surgery Basic KnowledgeDocument28 pagesCardiac Surgery Basic KnowledgeGinwong100% (1)
- Cardiac Surgery Made Ridiculously SimpleDocument23 pagesCardiac Surgery Made Ridiculously Simplelenovovonel1982No ratings yet
- 27 Ovarian Cystectomy Consent FormDocument3 pages27 Ovarian Cystectomy Consent FormsekyNo ratings yet
- Pathological FractureDocument92 pagesPathological FractureSeptyAuliaNo ratings yet
- Open Fracture Raju3Document72 pagesOpen Fracture Raju3Chowdhury Iqbal MahmudNo ratings yet
- Consent Transsphenoidal SurgeryDocument10 pagesConsent Transsphenoidal SurgeryAbhinav GuptaNo ratings yet
- A-Z of Neurosugery (April 2016 Update)Document13 pagesA-Z of Neurosugery (April 2016 Update)VamsiKrishnaChagalakondaNo ratings yet
- Mesenteric AngiographyDocument7 pagesMesenteric AngiographySleman M BashirNo ratings yet
- ER Tips and Tricks 2017 FINALforPDFDocument23 pagesER Tips and Tricks 2017 FINALforPDFmohamed zeegoNo ratings yet
- SXDocument126 pagesSXpalak32No ratings yet
- Humerus Fracture NotesDocument20 pagesHumerus Fracture Notes돼끼빈No ratings yet
- Avoiding Common Errors in The Emergency Department-801-1002Document200 pagesAvoiding Common Errors in The Emergency Department-801-1002Hernando CastrillónNo ratings yet
- Advance Trauma Life Support: Andi Siswandi, MD Surgeon Malahayati University, Medicine FacultyDocument76 pagesAdvance Trauma Life Support: Andi Siswandi, MD Surgeon Malahayati University, Medicine Facultyhari dorismanNo ratings yet
- Divine Intervention Episode 24 Surgery Shelf ReviewDocument118 pagesDivine Intervention Episode 24 Surgery Shelf ReviewPedro Weslley100% (3)
- Divine Intervention Episode 24 Surgery Shelf ReviewDocument118 pagesDivine Intervention Episode 24 Surgery Shelf ReviewrudolphNo ratings yet
- Redbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFDocument323 pagesRedbook - ASSESSMENT AND MANAGEMENT OF TRAUMA PDFrizka100% (1)
- Cardiac Anesthesia Made Ridiculously SimpleDocument17 pagesCardiac Anesthesia Made Ridiculously SimplecoolzygoteNo ratings yet
- Clinical Scenario 10 SummaryDocument1 pageClinical Scenario 10 SummaryMarios GhobrialNo ratings yet
- Amputation: Lesson Plan On ONDocument7 pagesAmputation: Lesson Plan On ONdhanasundariNo ratings yet
- Approach For Poly-Trauma PatientDocument63 pagesApproach For Poly-Trauma PatientvadimmadanNo ratings yet
- Computerized Tomography (CT) Scan: Indication Abnormal ResultsDocument7 pagesComputerized Tomography (CT) Scan: Indication Abnormal ResultsVanessa VillanuevaNo ratings yet
- Oet New Reading 1Document9 pagesOet New Reading 1Sanchit AbrolNo ratings yet
- Cardiac CardiacResynchronizationTherapyDefibrillator 0117 EngDocument3 pagesCardiac CardiacResynchronizationTherapyDefibrillator 0117 EngStella PraphulKumarNo ratings yet
- Lumbar Laminectomy Surgery For Spinal StenosisDocument15 pagesLumbar Laminectomy Surgery For Spinal StenosisElizabeth Liles MartinezNo ratings yet
- Presentation2.Ppt P&CDocument38 pagesPresentation2.Ppt P&CElla CaroNo ratings yet
- (Erdn) Compartment SyndromeDocument4 pages(Erdn) Compartment SyndromeKyl M. SrrcNo ratings yet
- Pectus Carinatum Leaflet PIAG 212Document9 pagesPectus Carinatum Leaflet PIAG 212MellNo ratings yet
- Week 9 Case Study 9 Chir13009Document7 pagesWeek 9 Case Study 9 Chir13009api-479754549No ratings yet
- Case Report Jai 3Document8 pagesCase Report Jai 3EACMed Nursing Station 5th FloorNo ratings yet
- Consent NeuroendosDocument7 pagesConsent NeuroendosAbhinav GuptaNo ratings yet
- Perioperative Care For CABG PatientsDocument32 pagesPerioperative Care For CABG PatientsAya EyadNo ratings yet
- Chapter 136 Pediatric Urologic and Gynecologic DisordersDocument12 pagesChapter 136 Pediatric Urologic and Gynecologic Disordersemergency.fumcNo ratings yet
- Westmead Obstetric AnaestheDocument85 pagesWestmead Obstetric Anaesthesum75No ratings yet
- Non-Operating Room Anesthesia (NORA) : A Beginner's GuideDocument26 pagesNon-Operating Room Anesthesia (NORA) : A Beginner's GuidepaulaNo ratings yet
- MeatoplastyDocument7 pagesMeatoplastyAndyNo ratings yet
- Book-for - A دوسية من دكتور المقاصدDocument63 pagesBook-for - A دوسية من دكتور المقاصدAli Toma HmedatNo ratings yet
- LAS4B5Document4 pagesLAS4B5jovert davidNo ratings yet
- Low Back Pain: TriageDocument12 pagesLow Back Pain: TriageabidhashamNo ratings yet
- Case Study Hip FractureDocument9 pagesCase Study Hip FractureufuNo ratings yet
- NYSORA Hazdics RegionalDocument8 pagesNYSORA Hazdics RegionalAishu BNo ratings yet
- IntroductionDocument5 pagesIntroductionFarhan YulmiadiNo ratings yet
- Cardiovascular MCQsDocument23 pagesCardiovascular MCQssb medexNo ratings yet
- Indirani College of Nursing: AmputationDocument7 pagesIndirani College of Nursing: AmputationdhanasundariNo ratings yet
- Surgery Emergencies: Multiple Trauma: Yonathan Adi PurnomoDocument66 pagesSurgery Emergencies: Multiple Trauma: Yonathan Adi Purnomowaraney palitNo ratings yet
- Anterior Cord SyndromeDocument8 pagesAnterior Cord SyndromeJanine Erika Julom BrillantesNo ratings yet
- Principles Fracture ManagementDocument88 pagesPrinciples Fracture ManagementYauffa Hanna Elt MisykahNo ratings yet
- Exams MedsurgDocument29 pagesExams MedsurgUy Jezrielle MicahNo ratings yet
- Testicular Torsion: A Urological EmergencyDocument4 pagesTesticular Torsion: A Urological EmergencycorsaruNo ratings yet
- December 2008final FRCA VivaDocument43 pagesDecember 2008final FRCA Vivajahangirealam100% (2)
- Case Study On Head InjuryDocument15 pagesCase Study On Head InjuryPriya SinghNo ratings yet
- Abdominal Mass Removal: Hugh H. Allen, M.DDocument6 pagesAbdominal Mass Removal: Hugh H. Allen, M.DAbbyKristekNo ratings yet
- Wilson SurgeryDocument83 pagesWilson SurgeryRada NemirovskiNo ratings yet
- Medical Surgical Nursing Review 1Document422 pagesMedical Surgical Nursing Review 1jeshemaNo ratings yet
- Procedural Skill by NPDocument92 pagesProcedural Skill by NPsankethg93No ratings yet
- Eng Inform Consent LP May09Document4 pagesEng Inform Consent LP May09clinfoxNo ratings yet
- CVC Catheter-Consent OnlyDocument4 pagesCVC Catheter-Consent OnlyRia Gita PratiwiNo ratings yet
- Orthopaedic Surgery Study Guide FOR Medical Students, R1S and R2SDocument17 pagesOrthopaedic Surgery Study Guide FOR Medical Students, R1S and R2SlanghalilafaNo ratings yet
- Osna/Cour International Scholarship Application: Md/Do Resident/PhysicianDocument4 pagesOsna/Cour International Scholarship Application: Md/Do Resident/PhysicianRajiv NegandhiNo ratings yet
- Adult Spina BifidaDocument13 pagesAdult Spina BifidaRajiv NegandhiNo ratings yet
- Posna International Educational Scholarship Recommendation FormDocument2 pagesPosna International Educational Scholarship Recommendation FormRajiv NegandhiNo ratings yet
- Gentamycin BeadsDocument3 pagesGentamycin BeadsRajiv NegandhiNo ratings yet
- Mfo AbstractDocument1 pageMfo AbstractRajiv NegandhiNo ratings yet
- Posna International Educational Scholarship Recommendation FormDocument3 pagesPosna International Educational Scholarship Recommendation FormRajiv NegandhiNo ratings yet
- Help CfponsetiDocument32 pagesHelp CfponsetiRajiv NegandhiNo ratings yet
- Gentamycin BeadsDocument3 pagesGentamycin BeadsRajiv NegandhiNo ratings yet
- Lateral Condyle 2Document10 pagesLateral Condyle 2Rajiv NegandhiNo ratings yet
- Antibiotic BeadsDocument7 pagesAntibiotic BeadsRajiv NegandhiNo ratings yet
- Gait AnalysisDocument10 pagesGait AnalysisRajiv NegandhiNo ratings yet
- Christopher W. DiGiovanni ArticleDocument10 pagesChristopher W. DiGiovanni ArticleRajiv NegandhiNo ratings yet
- Info For The Limited Registration App FormDocument2 pagesInfo For The Limited Registration App FormRajiv NegandhiNo ratings yet
- 517Document7 pages517Rajiv NegandhiNo ratings yet
- Notice For Renewal of RegistrationDocument1 pageNotice For Renewal of RegistrationRajiv NegandhiNo ratings yet
- Limited Registration - NoteDocument1 pageLimited Registration - NoteRajiv NegandhiNo ratings yet
- Limited Registration Application FormDocument3 pagesLimited Registration Application FormRajiv NegandhiNo ratings yet
- Gentamycin BeadsDocument3 pagesGentamycin BeadsRajiv NegandhiNo ratings yet
- Posicon 2012 Posicon 2012Document6 pagesPosicon 2012 Posicon 2012Rajiv NegandhiNo ratings yet
- BIOL 3121 - Lecture 13 - 081116Document91 pagesBIOL 3121 - Lecture 13 - 081116Sara HuebnerNo ratings yet
- Question Bank Respiratory SystemDocument13 pagesQuestion Bank Respiratory SystemDK Meerut statusNo ratings yet
- Natural Products Chemistry: Indian Institute of Integrative Medicine, JammuDocument2 pagesNatural Products Chemistry: Indian Institute of Integrative Medicine, JammuPratik VaghelaNo ratings yet
- A Review On Potential Toxicity of Artificial Sweetners Vs Safety of SteviaDocument13 pagesA Review On Potential Toxicity of Artificial Sweetners Vs Safety of SteviaAlexander DeckerNo ratings yet
- Instant Download Business Communication 16th Edition Lehman Test Bank PDF Full ChapterDocument32 pagesInstant Download Business Communication 16th Edition Lehman Test Bank PDF Full Chapterarthrosisretake8hro100% (8)
- Ovulation CalanderDocument2 pagesOvulation CalanderBN NGNo ratings yet
- Jagaroo & Santangelo - Neurophenotypes Advancing Psychiatry and Neuropsychology 2016Document305 pagesJagaroo & Santangelo - Neurophenotypes Advancing Psychiatry and Neuropsychology 2016Jaime Fernández-Aguirrebengoa100% (1)
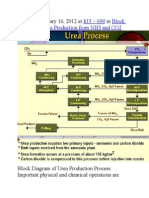
- Published January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2Document9 pagesPublished January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2himanshuchawla654No ratings yet
- Weekly Home Learning Plan: Day/Time Learning Competency Learning Tasks Mode of DeliveryDocument4 pagesWeekly Home Learning Plan: Day/Time Learning Competency Learning Tasks Mode of DeliveryEricha SolomonNo ratings yet
- 16S RRNA Gene Sequencing For Bacterial IdentificationDocument4 pages16S RRNA Gene Sequencing For Bacterial IdentificationBenjamin UcichNo ratings yet
- Multiple AlleleDocument3 pagesMultiple AlleleAdroit SangmaNo ratings yet
- Email To Professor SampleDocument6 pagesEmail To Professor SamplesimplecobraNo ratings yet
- 7 Pearson SquareDocument19 pages7 Pearson Squareapi-235944649No ratings yet
- Dihybrid Punnett SquaresDocument4 pagesDihybrid Punnett SquaresThomas Abich100% (1)
- Chapter 1Document4 pagesChapter 1Nikoleta RudnikNo ratings yet
- Taxonomy of Haematococcus PluvialisDocument2 pagesTaxonomy of Haematococcus PluvialisKomathi BalasupramaniamNo ratings yet
- Gen. Zoo. Final ReviewerDocument34 pagesGen. Zoo. Final ReviewerAshley FranciscoNo ratings yet
- His To PathologyDocument52 pagesHis To PathologyRathinaKumarNo ratings yet
- AP Biology Practice Exam: Section I: Multiple-Choice QuestionsDocument83 pagesAP Biology Practice Exam: Section I: Multiple-Choice QuestionsKamilla DzhanzakovaNo ratings yet
- Principles of Inheritance and Variations: By: Dr. Anand ManiDocument113 pagesPrinciples of Inheritance and Variations: By: Dr. Anand ManiIndu YadavNo ratings yet
- Third Stage Begg MechanotherapyDocument32 pagesThird Stage Begg MechanotherapyNaziya ShaikNo ratings yet
- ABCD Vocal Technique Handout PDFDocument9 pagesABCD Vocal Technique Handout PDFRanieque RamosNo ratings yet
- Chauhan2017mulberry SericultureDocument67 pagesChauhan2017mulberry SericultureNarasimha Murthy S VNo ratings yet
- Using STADEN For Sequence AssemblyDocument5 pagesUsing STADEN For Sequence AssemblyChristen Rune StensvoldNo ratings yet
- EuglenidDocument4 pagesEuglenidx456456456xNo ratings yet
- All CompleteDocument10 pagesAll CompleteNanep NanenanenaNo ratings yet
- Proposed Pre Final-1 Time Table With Weightage.. MPC, Bipc&Civils-AP&TsDocument17 pagesProposed Pre Final-1 Time Table With Weightage.. MPC, Bipc&Civils-AP&TsAbhiram muddanaNo ratings yet
- Microscopy and StainingDocument7 pagesMicroscopy and StainingDenmark ManlusocNo ratings yet
- NCERT Class 3 English Baloon ManDocument10 pagesNCERT Class 3 English Baloon ManAnonymous 9WyPyismNo ratings yet
- Pathomorophology. (Medicine, 3 Course)Document10 pagesPathomorophology. (Medicine, 3 Course)Joy JoyNo ratings yet